♦ Preoperative
Imaging
- Magnetic resonance imaging to assess need for neural element decompression (transoral odontoidectomy, enlargement of foramen magnum, C1 or subaxial laminectomies)
- Computed tomography with thin-cut reconstructions for bone depth and screw lengths, relationship of vertebral artery to C2 pedicle
Preoperative Care
- Patients with traumatic occipitocervical dislocation should be placed in halo.
- Patients with basilar invagination are frequently admitted before surgery and placed in traction to determine if odontoidectomy needed.
Equipment
- Occipital screw set and connector to secure rods to cervical construct, standard lateral mass system of choice, or
- Threaded Steinmann pin, double Songer cable (DePuy Spine Inc., Raynham, MA) for sublaminar wires, single Songer cable for occiput, BendMeister Stein-mann pin bender (Sofamor Danek, Memphis, TN)
- Halo adapter for Mayfield head holder and halo vest removal tools
Operating Room Set-up
- Somatosensory and motor evoked potential monitoring (optional)
- Fluoroscopy
Positioning
- Regular bed with rolls with head in Mayfield holder or Jackson table (Mizuho OSI) and foam or horseshoe headrest with traction
- If in halo, turn prone in halo vest, fix head to Mayfield with halo adapter, then remove the posterior part of the vest and posts.
- Head must be in neutral position; confirm with lateral fluoroscopy.
♦ Intraoperative
Exposure
- Subperiosteal exposure from inion to each lamina and lateral mass
- Decompression of neural elements if necessary
Screw-Rod Technique
- Place C1 lateral mass, C2 pedicle or pars screws, subaxial lateral mass screws as indicated
Placement of Occipital Screws (Fig. 91.1)
- Determine where the rods and connector will sit on the occipital bone.
- Mark the entry points for the screws in the occipital bone through the holes in the connector.
- Drill the pilot holes with Midas Rex AM-8 bit, then use a hand drill to the predetermined depth (usually 8 to 12 mm).
- Place appropriate sized screw.
Secure the Rods to the Screw Heads
- Torque-limited final tightener
- Consider cross-link for multiple subaxial levels.
Bone Graft
- Decorticate lateral masses, C1–C2 facet joint, and occiput.
- Lay cancellous iliac crest autograft or autograft over lateral masses and occiput, pack into facet joints
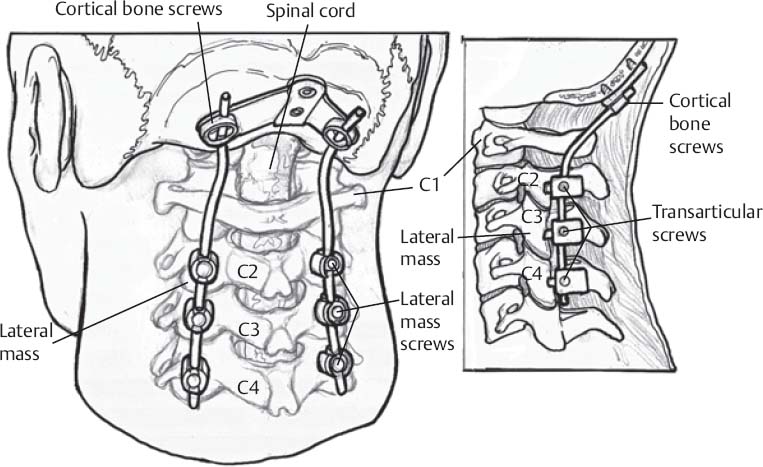
Fig. 91.1 Posterior and lateral views of occipitocervical instrumentation.
Only gold members can continue reading. Log In or Register to continue
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


