Fig. 1
Hind limb foot faults per second. Injured animals treated with a craniectomy only (TBI + C) have significantly more hind limb foot faults per second than naïve animals (Naïve). Injured animals treated with a craniectomy plus OTD (TBI + C + OTD) have a reduced number of hind limb foot faults per second, such that the foot faults are comparable (not statistically significant) to the number of foot faults per second by naïve animals. * p < 0.05 vs Naïve
Beam Balance Test
Naïve animals (Naïve, n = 6) subjected to the beam balance test were all able to walk on the beam for the entire time allotted, so the time to fall was 60 ± 0.0 s. However, injured animals treated with a craniectomy only (TBI + C, n = 3) had more difficulty remaining on the beam (time to fall: 43 ± 10.6 s); time to fall for injured animals treated with a craniectomy only was significantly lower than that of naïve animals (p < 0.05). Treatment with a craniectomy plus an OTD (TBI + C + OTD) improved their proprioception (no animals fell, time to fall: 60 ± 0.0 s) to that of the naïve group (p > 0.05) (Fig. 2a).
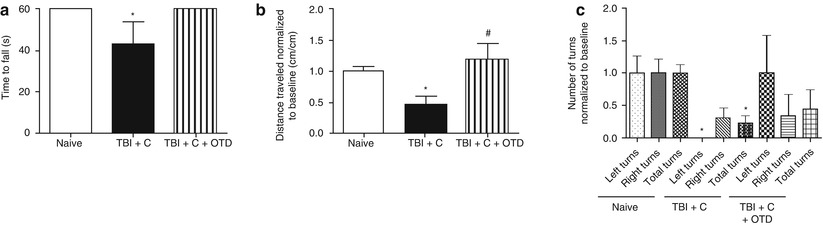
Fig. 2
Beam balance test. (a) Time to fall (s) was significantly lower for injured animals treated with a craniectomy (TBI + C) compared with naïve animals (Naïve). Injured animals treated with a craniectomy plus OTD (TBI + C + OTD) had a time to fall similar to naïve animals. (b) Distance traveled (normalized to the pretest baseline distance traveled, cm/cm) was significantly reduced in injured animals treated with a craniectomy only (TBI + C) compared with naïve animals. Treatment with a craniectomy plus OTD (TBI + C + OTD) significantly improved the distance traveled compared with animals treated with a craniectomy only. (c) Number of turns (normalized to the pretest baseline values) was significantly reduced in injured animals treated with a craniectomy only (TBI + C) for the number of left and total turns. Injured animals treated with a craniectomy plus OTD (TBI + C + OTD) improved the number of turns such that no significant difference was observed between naïve animals for the number of left and total turns. No difference was observed between the numbers of right turns between any of the groups. * p < 0.05 vs Naïve, # p < 0.05 vs TBI + C
In the 60 s given to naïve animals for walking on the beam, the distance traveled was 115 ± 65 cm. When normalized to the baseline distance traveled for each animal, the naïve group had a normalized distance traveled of 1.0 ± 0.08. Injured animals treated with a craniectomy only had a significantly lower normalized distance traveled (0.5 ± 0.12) compared with naïve animals (p < 0.05). But when injured animals are treated with a craniectomy and an OTD, the normalized distance traveled (1.2 ± 0.25) was significantly higher than injured animals treated with only a craniectomy (p < 0.05) and indistinguishable from naïve animals (p > 0.05) (Fig. 2b).
The number of turns, normalized to naïve values, for the naïve animals were 1.0 ± 0.26, 1.0 ± 0.21, and 1.0 ± 0.13 for the left, right, and total turns, respectively. Normalized number of turns for injured animals treated with a craniectomy only were 0.0 ± 0.00, 0.3 ± 0.16, and 0.2 ± 0.11 for the left, right, and total turns, respectively. Normalized number of turns for injured animals treated with a craniectomy only were 1.0 ± 0.58, 0.3 ± 0.33, and 0.4 ± 0.29 for the left, right, and total turns, respectively. Statistical significance was observed between the normalized number of turns for naïve animals and injured animals treated with craniectomy only for left and total turns (p < 0.05). All other intergroup comparisons were not statistically significant (p > 0.05) (Fig. 2c).
Discussion
The effect of craniectomy treatment for severe TBI on patient outcomes has been debated. Experimental evidence for the therapeutic benefits, including functional recovery, for craniectomy treatment of severe TBI in animal models has been thoroughly examined and primarily indicates that craniectomy is neuroprotective [6, 20]. However, the study by Floyd et al. [6] examined the effect of craniectomy position and found that slight differences in the position of the craniectomy can produce changes in cognitive performance in a rat TBI model. The results of Floyd et al. were mimicked in the study by Lee et al. [12], which also observed a correlation between the location of craniectomy and functional recovery. Clinical reports are also inconsistent on the effect of craniectomy and patient outcome; whereas several reports observed improved patient outcome after decompressive craniectomy [1, 9, 19], the HeADDFIRST [7] and DECRA [5] clinical trials found conflicting and/or inconclusive results of craniectomy treatment on patient outcome. While we wait for the results of the RESCUEicp trial, the need for a treatment of cerebral edema remains of the utmost importance. An OTD has been shown to improve survival rates of water intoxicated mice [14] and reduce brain edema in mice with TBI [15]. Herein, we hypothesized that direct osmotherapy via an OTD is more neuroprotective than craniectomy alone, improving functional outcomes after TBI in mice.
The neurological function of mice after TBI was examined via testing of sensorimotor, proprioception, and balance. The foot fault test found TBI to be associated with functional deficits in the hind limbs of injured animals treated with a craniectomy only compared with those of naïve animals. When injured animals are treated with a craniectomy and an OTD, the number of hind limb faults decreased such that it was not statistically different from the naïve animals. The beam balance test identified that TBI was associated with balance (time to fall) and motor deficits (reduced distance traveled and turning) in animals treated with a craniectomy only compared with naïve animals. When injured animals are treated with a craniectomy plus an OTD, balance is improved and motor deficits are reduced. These tests supported our hypothesis that craniectomy plus OTD (combined therapy) improves functional outcome better than craniectomy alone and further support the therapeutic benefits of direct osmotherapy.
Related posts:
 of Behavioral Deficits in Rodents Following Brain Injury Across Species, Gender, and Experimental Model
of Behavioral Deficits in Rodents Following Brain Injury Across Species, Gender, and Experimental Model
 Infarction After Aneurysmal Subarachnoid Hemorrhage
Infarction After Aneurysmal Subarachnoid Hemorrhage
 Volume Determination in Subarachnoid Hemorrhage Using Rats
Volume Determination in Subarachnoid Hemorrhage Using Rats
 Pretreatment Fails to Provide Neuroprotection Following a Surgically Induced Brain Injury Rat Model
Pretreatment Fails to Provide Neuroprotection Following a Surgically Induced Brain Injury Rat Model
 IGF-1 Reduced Rat Pup Germinal Matrix Hemorrhage
IGF-1 Reduced Rat Pup Germinal Matrix Hemorrhage
 Injection of Noncellular Cerebrospinal Fluid from Subarachnoid Hemorrhage Patient into Rat Ventricles Leads to Ventricular Enlargement and Periventricular Injury
Injection of Noncellular Cerebrospinal Fluid from Subarachnoid Hemorrhage Patient into Rat Ventricles Leads to Ventricular Enlargement and Periventricular Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


