Front Neurol Neurosci. Basel, Karger, 2014, vol 33, pp 69-81 (DOI: 10.1159/000351892)
______________________
Epidemiology of Transient Ischemic Attack
Yoshihiro Kokubo
Department of Preventive Cardiology, National Cerebral and Cardiovascular Disease, Osaka, Japan
______________________
Abstract
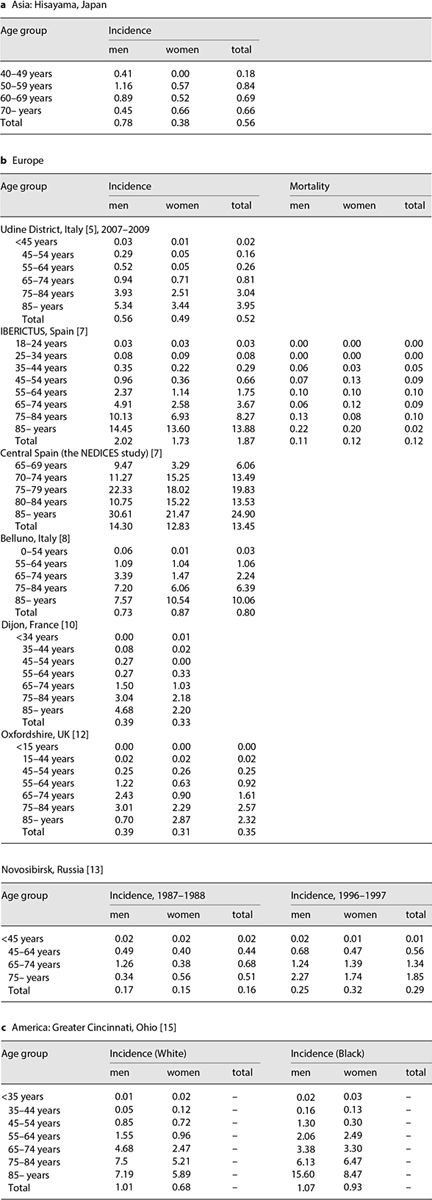
Few epidemiologic data are available regarding the prevalence and incidence of transient ischemic attack (TIA). Here, the incidence of TIA and that of subsequent stroke events were reviewed. The incidences of TIA in Europe were 0.52-2.37 and 0.05-1.14 in men and women aged 55-64, 0.94- 3.39 and 0.71-1.47 in those aged 65-74, and 3.04-7.20 and 2.18-6.06 in those aged 75-84, respectively. The corresponding incidences are similar in the United States, and lower in Japan. Higher incidences were revealed in men compared with women. The incidence of TIA increased very markedly with age, regardless of race or gender. The evidence of risk factors for TIA excluding ischemic strokes is very limited. The ABCD/ABCD2 score was developed to predict individual risk and to triage patients on the first presentation. In prognostic TIA, the crude rate of stroke risks (%) for general populations were 1.7, 4.8, 6.6, 8.5, and 11.4 at 2 days, 1 week, 1 month, 3 and 6 months, whereas those for hospital patients were 13.7 and 12.4 at 1 and 3 months, respectively. There is very limited evidence of an association between a family history of stroke and the incidence of stroke after TIA, which showed that family history of stroke does not predict the risk of ischemic stroke after TIA. There is also limited evidence of seasonal variation in TIA incidence. TIAs were reported to be most frequent in autumn or spring and less common in winter or spring to summer, and most frequent on Mondays. There seems to be no consensus regarding seasonal differences in TIA incidence.
Copyright © 2014 S. Karger AG, Basel
Transient ischemic attack (TIA) is an acute episode of temporary neurologic impairment lasting <24 h, caused by focal ischemia in the brain or retina. TIAs are variable in duration, commonly lasting from 5 to 60 min, but they occasionally last as long as 24 h, but may leave no persistent neurological deficit [1]. According to the recent American Heart Association/American Stroke Association diagnostic recommendations, TIA patients should undergo a neuroimaging evaluation within 24 h of symptom onset. Patients who have experienced a TIA are at high risk of stroke. However, there are few epidemiologic data on TIA, especially reviews of the incidence and prognostic value of TIAs. In this review, I will focus on the incidence of TIA and subsequent stroke events from an epidemiological point of view.
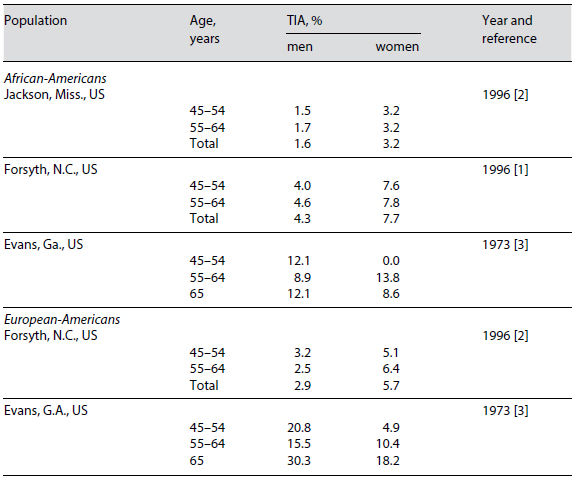
Table 1. Prevalence of TIA according to age, sex, and race/ethnic group
Prevalence and Incidence of Transient Ischemic Attack
The prevalence of TIA according to age, sex, and race/ethnic group is shown in table 1 [2, 3]. Among African-Americans, the prevalence of TIA does not seem to increase according to age in both men and women. According to the Atherosclerosis Risk in Communities (ARIC) Study, the prevalence of TIA in African-American men and women per 1,000 persons was 1.5-1.7 and around 3.2 in Jackson, Miss., but 4.0-4.6 and 7.6-7.8 in Forsyth, N.C., respectively [2]. However, in Evans County, Ga., the prevalence of TIA in the age groups 45-54, 55-64, and 65+ years was 12.1, 8.9, and 12.1 in men and 0, 13.8, and 8.6 in women per 1,000 persons, respectively [3]. These prevalence results are much higher than those obtained in Jackson and Forsyth. The data for Jackson and Forsyth are from 1996, which is 23 years after the Evans data. These two sets of data may not be compared simply because of a different generation.
In the ARIC study, the diagnosis of TIA was categorized as definite for a sudden onset of transient limb paralysis, with or without other signs, lasting up to 24 h and leaving no significant deficit; probable for other transient focal neurologic deficits lasting up to 24 h; possible for a less clear-cut history of symptoms or non-focal symptoms, or vague for anxiety and/or emotional symptoms. Evans County, is located in ‘the Stroke Belt’ in the south-eastern United States, which shows relatively higher stroke incidence. Therefore the prevalence of TIA in Evans County seems to be greater than in other areas.
In a European-American population in Forsyth, the prevalence of TIA was 2.9 and 5.7 in men and women per 1,000 persons, respectively. In Evans, the TIA prevalence of a European-American population was 20.8, 15.5, and 30.3 in men and 4.9, 10.4, and 18.2 in women per 1,000 persons according to the 45-54, 55-64, and 65 or older (65+) age groups, respectively. The prevalence of TIA tends to increase according to age in both men and women.
The Hisayama study examined the prevalence of TIA in the Japanese population [4]. The prevalence of TIA in the Hisayama study was 4.9 per 1,000 persons [4], less than half that in the European-American population in Evans. (13.8 per 1,000 persons) [3]. The etiology of incident TIA in Japan may be different from that in Western countries. Among the Hisayama participants with TIA, 11 subsequent cerebral infarctions were observed; they were diagnosed as 6 lacunar infarctions, 3 embolisms, and 2 atherothromboses by clinical and/or pathological finding or autopsy. The ARIC study showed that TIA due to atherosclerosis was attributable to myocardial infarction in 57% and to stroke in 38% of mortality patients (n = 37) [2]. TIAs due to atherosclerosis (which is usually of carotid artery origin) are estimated to be less common in Japan than in Western countries, and lacunar stroke might be important as an etiology of TIA in Japan [2].
As illustrated in figure 1 [4–11] and table 2, [4, 5, 7, 8, 10, 12–15] the Hisayama study found that the average incidence of the first TIA was 0.78 and 0.38 per 1,000 person-years in men and women, respectively [4]. According to community studies in the US, the average incidence rate for the first TIA was 0.31 per 1,000 personyears (0.93 per 1,000 person-years for those aged >65 years) in Rochester, Minn. [16], and 1.1 per 1,000 person-years in Seal Beach, Californian community [11], where the incidence of all strokes and TIA with previous cerebrovascular events were 7.1 and 1.4 per 1,000 person-years during the period 1963-1967, respectively. The incidence for men was 9.7, 1.7 times the incidence of 5.7 for women per 1,000 person-years.
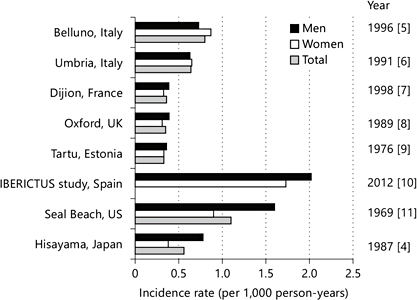
Fig. 1. Incidence of TIA in several countries.
The incidence rate of TIA in Belluno, Italy, was 0.80 per 1,000 person-years, and the incidence was non-significantly higher in women than in men (0.73 per 1,000, 95% confidence interval, CI: 0.57-0.91 in men, and 0.87 per 1,000, 95% CI: 0.70-1.06 in women) [5]. After adjustment for the European population, the overall incidence rate decreased to 0.58 per 1,000 inhabitants per year. The mean age of new TIA patients was 73.9 years, and the women were significantly older than the men (p < 0.001). The SEPIVAC study of a population in Umbria, Italy revealed a crude rate of 0.64 per 1,000 per year (95% CI: 0.52-0.78), and the authors reported that the rate adjusted to the European population is 0.42 (95% CI: 0.33-0.54) [6]. It is of note that in the Umbria population, one third of the new TIA patients was cared for at home [6]. In Tartu, Estonia, USSR, from 1970 to 1973, the incidence of TIA was 0.33 per 1,000 person-years [9], and the mortality rate for stroke for this population was 0.98 per 1,000 person-years [9]. The Italian and Estonian data on the incidence of TIA, its dependence on age and sex, and mortality rate are close to the corresponding data reported from other countries.
The Oxfordshire Community Stroke Project showed that the crude TIA incidence rate and the TIA rate standardized to the 1981 population of England and Wales were 0.35 and 0.42 per 1,000 person-years, respectively [8]. The incidence of TIA increased sharply with increasing age, and the overall incidence in men was very similar to that in women (incidence ratio 1.3). However, in middle age, men were 2.6 times more likely to suffer a TIA.
Table 2. Incidence and mortality of TIA according to age, sex, and race/ethnic group (per 1,000 person-years)
In Dijon, France, crude TIA incidence rates of 0.39 and 0.33 per 1,000 person-years were revealed for men and women, respectively [7]. The mean age of first-ever TIA was higher in women (71.8 years) than in men (70.4 years). CT scans were performed in 97% of the cases. These incidence rates were similar to those of previous population-based studies, such as Belluno [5
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


