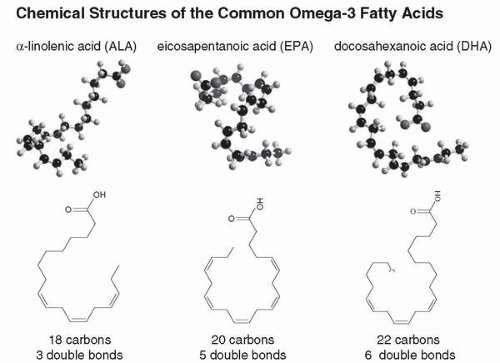
 Figure 4.1 • Note the recurring double bonds at every third carbon atom. The presence of multiple double bonds in polyunsaturates, such as omega-3 fatty acids (n-3s) leads to a very kinked and flexible molecule. This flexibility permits increased molecular motion, which is why polyunsaturates (e.g., n-3 and n-6 oils) are liquid at room temperature and produce a more fluid cell membrane. Saturated fat, with no double bonds, is a straight and rigid molecule. Saturated fats are solids at room temperature and tend to produce less fluid cell membranes. |
demonstrated in various cell types and tissues in the periphery (20,22), and it presumably occurs in brain as well. The established mood stabilizers, lithium and valproate also appear to inhibit different aspects of signal transduction related to the PI system (21,23). Thus, one possible mechanism for the apparent mood stabilizing and antidepressant action of the omega-3 fatty acids is this dampening effect on signal transduction.
TABLE 4.1 Potential Mechanisms of Action of Omega-3 Fatty Acids in Mood Disorders | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
TABLE 4.2 Comparison of Controlled Treatment Studies of Omega-3s in Bipolar Disorder | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
conflicting findings. For example, in three of the four studies, patients with different subtypes of bipolar disorder were included (55,59,60). The fourth study (61) recruited only patients with bipolar disorder type I. It is conceivable that patients with bipolar type I may respond differently to omega-3 fatty acids from patients with bipolar type II. Unfortunately, the sample sizes of these studies appear too small to be able to do valid analyses of bipolar types I and II separately. Other methodologic differences include differing mood states at baseline.
review the old and the new lines of evidence supporting a role for the omega-3 fatty acids in major depression.
Related posts:
 Complementary and Alternative Medicine in Society: An Introduction
Complementary and Alternative Medicine in Society: An Introduction
 Evaluating the Data: Limitations of Research and Quality Assurance Issues Regarding Natural Remedies
Herbal Remedies for Anxiety and Insomnia: Kava and Valerian
Evaluating the Data: Limitations of Research and Quality Assurance Issues Regarding Natural Remedies
Herbal Remedies for Anxiety and Insomnia: Kava and Valerian
 Therapeutic Potential of Melatonin in Sleep and Circadian Disorders
Acupuncture for the Treatment of Psychiatric Disorders
Homeopathy and Its Applications in Psychiatry
Therapeutic Potential of Melatonin in Sleep and Circadian Disorders
Acupuncture for the Treatment of Psychiatric Disorders
Homeopathy and Its Applications in Psychiatry
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


