Ontogeny of Sleep
Paul R. Carney
James D. Geyer
INTRODUCTION
After the discovery of electroencephalographic waves in dogs by the English physician Caton (1) in 1875, and of the alpha waves from scalp electroencephalogram (EEG) by the German physician Hans Berger (2) in 1929, researchers began to obtain recordings of brain electrical activity from fetuses and infants. Lindsley (3) recorded fetal cardiac and cerebral electrical activity, and Hughes (4) performed EEG studies in premature infants. Following the discovery of rapid eye movement (REM) sleep by Aserinsky and Kleitman (5) in 1953, it was also noted that REM and nonrapid eye movement (NREM) sleep could be differentiated by 30 weeks conceptional age (CA) (6). With improved ventilation and neonatal intensive care, healthy 23 to 30 weeks CA infants are more likely to survive without hypoxic ischemic injury, and state differentiation could be identified as early as 27 weeks CA. Sleep and wakefulness patterns develop rapidly during the prenatal and newborn period and continue to change during the first years of life. Sleep patterns then remain stable and without significant changes until late adulthood.
DIFFERENTIATION OF SLEEP AND WAKEFULNESS STATES
Newborns have a polyphasic sleep pattern and spend about two-thirds of their time sleeping during the first weeks of life. This polyphasic sleep pattern gradually changes into the monophasic adult pattern (7). Brain electrical activity, body and eye movements, and respiratory patterns are used to differentiate sleep and wake states. On falling asleep, a normal newborn enters into REM sleep, also referred to as active sleep. Random spontaneous movements of arms, legs, and facial muscles accompany active sleep. In premature infants (<37 weeks CA), it can be difficult to distinguish REM from wakefulness. Body movements and brainstem electrical activity are present at approximately 10 weeks CA, and cerebral cortical activity can be identified at 17 weeks CA. Rhythmic cycling body movements begin at 20 to 24 weeks CA (6). High-voltage slow waves and low-voltage 8- to 14-Hz activity is separated by 20-to 30-second intervals of low-voltage nearly isoelectric background. This EEG activity occurs in an asynchronous fashion over the two hemispheres and is usually accompanied by irregular respiration and irregular eye movements. The discontinuous EEG pattern is often referred to as tracé discontinu. Irregular respiration and occasional eye movements accompany trace discontinu sleep.
Between 27 and 30 weeks CA, the EEG is usually discontinuous and background activity is asynchronous. With increasing age, the periods between bursts become increasingly shorter. Central and temporal sharp wave transients are common features during this age. Posterior predominant delta waves with superimposed 14- to 24-Hz activity called delta brushes appear. During quiet sleep, the EEG is discontinuous and eye movements are rare. During active sleep, continuous delta or theta-delta activity predominates. Cardiac and respiratory rhythms are more regular and apparent during quiet sleep than during active sleep. At 33 to 34 weeks CA, muscle tone decreases during active sleep relative to quiet sleep (8). The terms indeterminate sleep and transitional sleep are used to describe periods of sleep that cannot be classified as either quiet sleep or active sleep.
Between 30 and 33 weeks CA, a low-voltage, mixedfrequency, and nearly continuous EEG pattern occurs during active sleep. However, during quiet sleep, the EEG remains discontinuous, and bursts of high-voltage delta activity followed by 10 seconds of low-voltage activity can be observed. Temporal and frontal sharp transients
and delta brushes remain the prominent EEG patterns. With the emergence of distinctive active and quiet sleep patterns, transitional sleep also becomes more prominent at 32 to 33 weeks CA (9). At 34 weeks CA, NREM-REM cycle duration is approximately 45 minutes, which increases to 60 minutes at 38 weeks CA or full-term infant.
and delta brushes remain the prominent EEG patterns. With the emergence of distinctive active and quiet sleep patterns, transitional sleep also becomes more prominent at 32 to 33 weeks CA (9). At 34 weeks CA, NREM-REM cycle duration is approximately 45 minutes, which increases to 60 minutes at 38 weeks CA or full-term infant.
Between 33 and 37 weeks CA, features including smiling, grimaces, and body twitches are present during active sleep. By 37 weeks CA, active sleep is well differentiated. Medium-voltage and continuous EEG, REMs, irregular breathing patterns, muscle atonia, and phasic twitches of the face and extremities are present. During quiet sleep, breathing patterns are regular and body movements are rare. The EEG during quiet sleep shows an alternating pattern (traceé alternant) in which 1- to 10-second bursts of moderate- to high-amplitude delta activity alternate with 5- to 10-second intervals of low-voltage, mixedfrequency theta activity. Beginning at approximately 37 weeks CA, the EEG becomes more continuous with increasing age.
DEVELOPMENT OF SLEEP-WAKE CYCLE
Infancy
Infants spend about one-third of the time in the awake state. The remaining two-thirds (∽16 hours) of time is equally divided between NREM and REM sleep. Sleep-wake states alternate in 3- to 4-hour cycles, with randomly timed phases of wakefulness, active sleep, and quiet sleep. Within the first month following birth, sleep-wake phase organization begins to adapt to the light-dark cycle and to the associated social cues. The circadian rhythm of temperature appears first. Soon after birth, circadian wake rhythm then appears (∽day 45 of life). Circadian sleep rhythm appears around day 56 of life (10). By 10 to 12 weeks of age, the development of neural systems produces a steady diurnal distribution of sleep and wake.
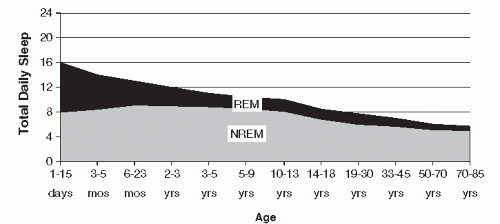 FIGURE 7-1 Changes in duration of NREM and REM sleep with age. (Adapted from Roffwarg HP, Munzio JN, Dement WC. Ontogenetic development of the human sleep-dream cycle. Science. 1966;152:604-619, with permission.) |
During the first 3 months of life, infants spend 50% of their sleep time in REM (active sleep) and 50% in NREM (quiet sleep). The proportion of sleep in REM and NREM changes dramatically during the first year of life. Sleep time declines to 13 hours at 1 year of life. REM sleep declines from 7 to 8 hours at birth to 6 hours by 6 months of life and then to 4 to 5 hours by 1 year of life. During the first month of life, sleep-onset REM occurs two-thirds of the time, declining to 20% by 6 months of life. At term, sleep-onset REM occurs only occasionally (9,11). With a steady decline in the proportion of REM sleep, NREM sleep becomes more predominant during the first half of sleep, and REM sleep predominates during the latter half of the sleep cycle. The latency before entering REM sleep gradually increases during the first year. The REM-NREM cycle length is between 60 to 70 minutes during the first year of life. By 4 to 5 years of age, the cycle length gradually increases to 90 minutes. By 10 years of life, total REM sleep resembles adult proportions of approximately 20% to 25% of total sleep time (TST), with the child averaging 9 hours of total sleep in a single nocturnal sleep period (12) (Fig. 7-1).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


