Chapter 16
Oral Appliances and Surgical Techniques for Obstructive Sleep Apnea Syndrome Therapy
This chapter is based on a recent overview of the treatment of the obstructive sleep apnea syndrome (OSAS) by oral appliances (OAs) and upper airway surgery1 with additional figures and videos.
Oral Appliances
OAs are widely used for the treatment of mild to moderate OSAS, both as primary therapy and as an alternative for patients who are unwilling or unable to tolerate continuous positive airway pressure (CPAP;  Video 16.1).2 There are currently a large number of different OAs available for the treatment of OSAS (Fig. 16.1;
Video 16.1).2 There are currently a large number of different OAs available for the treatment of OSAS (Fig. 16.1;  Videos 16.2 to 16.5). OAs increase the size of the upper airway by advancing either the mandible or the tongue. Mandibular advancement OAs are most widely used and employ traditional dental techniques to attach the OA to one or both dental arches. Construction usually requires dental impressions, bite registration (
Videos 16.2 to 16.5). OAs increase the size of the upper airway by advancing either the mandible or the tongue. Mandibular advancement OAs are most widely used and employ traditional dental techniques to attach the OA to one or both dental arches. Construction usually requires dental impressions, bite registration ( Video 16.6) and fabrication by a dental laboratory. Some OAs are available in a prefabricated form and are sometimes referred to as boil and bite. These can be either fitted by patients themselves or molded to patients’ teeth in an office setting. More recently OAs have been developed with an adjustable hinge that allows progressive advancement of the mandible after initial construction until the optimal mandibular position is achieved (
Video 16.6) and fabrication by a dental laboratory. Some OAs are available in a prefabricated form and are sometimes referred to as boil and bite. These can be either fitted by patients themselves or molded to patients’ teeth in an office setting. More recently OAs have been developed with an adjustable hinge that allows progressive advancement of the mandible after initial construction until the optimal mandibular position is achieved ( Video 16.7). The amount of anterior posterior mandibular movement and the speed with which this can be changed varies considerably between patients. The other major type of OA available is the tongue retainer, which keeps the tongue in an anterior position during sleep by means of negative pressure in a soft plastic bulb. It can be used in edentulous patients and is the OA of choice for patients with no teeth, limited anterior posterior mandibular movement, or an extremely large tongue. Patients should be assessed before OA treatment and should not have major active periodontal disease. Dental restorations should ideally be completed before treatment (
Video 16.7). The amount of anterior posterior mandibular movement and the speed with which this can be changed varies considerably between patients. The other major type of OA available is the tongue retainer, which keeps the tongue in an anterior position during sleep by means of negative pressure in a soft plastic bulb. It can be used in edentulous patients and is the OA of choice for patients with no teeth, limited anterior posterior mandibular movement, or an extremely large tongue. Patients should be assessed before OA treatment and should not have major active periodontal disease. Dental restorations should ideally be completed before treatment ( Video 16.8). Patients should be provided with information concerning the efficacy and side effects of OAs, and written consent should be obtained (
Video 16.8). Patients should be provided with information concerning the efficacy and side effects of OAs, and written consent should be obtained ( Video 16.9).
Video 16.9).
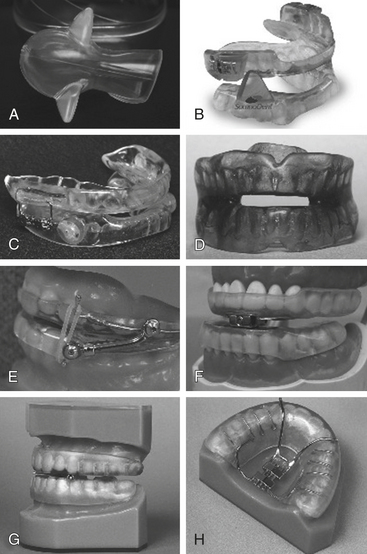
FIGURE 16.1 Different types of oral appliances used for the treatment of obstructive sleep apnea syndrome. A, AveoTSD (Innovative Health Technologies, Christchurch, New Zealand). B, SomnoDent (SomnoMed, Denton, TX). C, PM Positioner Adjustable PM Positioner (Wyoming, MI). D, Monoblock (Courtesy M. Marklund). E, Herbst (Great Lakes Orthodontics, Tonawanda, NY). F, MDSA (Medical Dental Sleep Appliance, R.J. and V.K. Bird, Australia). G, Klearway lateral view (Great Lakes Orthodontics, Tonawanda, NY). H, Klearway hinge view (Great Lakes Orthodontics, Tonawanda, NY). (Reproduced with permission of the European Respiratory Society. From Fleetham JA, Almeida FR. Oral appliances. Eur Respir Mon. 2010;50:267-285. http://dx.doi.org/10.1183/1025448x.00025209.)
The majority of OAs are designed to maintain the mandible and/or tongue in a protruded posture, thereby preventing upper airway obstruction during sleep. Several studies have demonstrated an increase in the anteroposterior diameter of the upper airway following OA insertion (Fig. 16.2). This increase was predominantly in the oropharynx and hypopharynx, but some studies have also suggested an effect on the velopharynx (Figs. 16.3 and 16.4). There is increasing evidence that OAs significantly improve snoring, daytime sleepiness, quality of life, systemic hypertension, and indices of sleep-disordered breathing. There are varying degrees of improvement in sleep-disordered breathing and side effects with different OAs. A variety of predictors of OA treatment success have been proposed. However, there is considerable overlap between good and poor treatment responses with all these variables. The utility of any treatment recommendation based on clinical features, OSAS severity, or upper airway anatomical characteristics requires prospective validation.
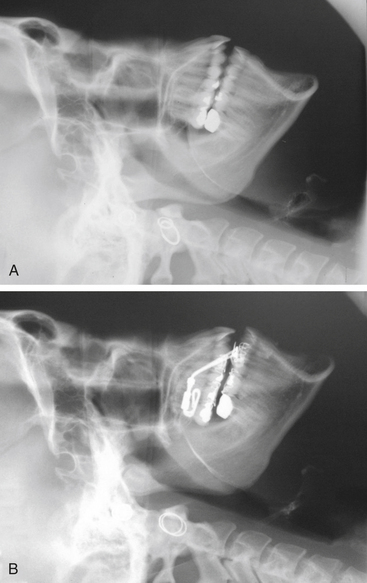
FIGURE 16.2 Lateral cephalometry of a male patient without (A) and with (B) a mandibular advancement oral appliance. Note the advancement of the mandible and an increase in the size of the velopharynx with the mandibular advancement oral appliance. (Reproduced with permission of the European Respiratory Society. From Fleetham JA, Almeida FR. Oral appliances. Eur Respir Mon. 2010;50:267-285. http://dx.doi.org/10.1183/1025448x.00025209)
Related posts:
 1: Narcolepsy—Unequivocal Diagnosis After Split-Screen, Video-Polysomnographic Analysis of a Prolonged Cataplectic Attack
1: Narcolepsy—Unequivocal Diagnosis After Split-Screen, Video-Polysomnographic Analysis of a Prolonged Cataplectic Attack
 4: Isolated Sleep Paralysis: An REM-“Sleep” Polysomnographic Phenomenon as Documented With Simultaneous Clinical and Electrophysiological Assessment
4: Isolated Sleep Paralysis: An REM-“Sleep” Polysomnographic Phenomenon as Documented With Simultaneous Clinical and Electrophysiological Assessment
 Motor Disorders During Sleep
Motor Disorders During Sleep
 Polysomnographic Recording Technique
Polysomnographic Recording Technique
 Specialized Techniques
Specialized Techniques
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


