6 Other Tumors of the Cerebellopontine Angle
 Neurinomas of the Facial Nerve
Neurinomas of the Facial Nerve
 Neurinomas of the Trigeminal Nerve
Neurinomas of the Trigeminal Nerve
 Neurinomas of the Glossopharyngeal Nerve
Neurinomas of the Glossopharyngeal Nerve
 Meningiomas
Meningiomas
 Epidermoid Cysts (Cholesteatomas)
Epidermoid Cysts (Cholesteatomas)
 Choroid Plexus Papillomas
Choroid Plexus Papillomas
 Arachnoid Cysts
Arachnoid Cysts
Neurinomas of the Facial Nerve
Case 1 (Fig. 6.1)
Diagnosis | Neurinoma of the facial nerve |
Approach | Retromastoid transmeatal |
Result | Total resection |
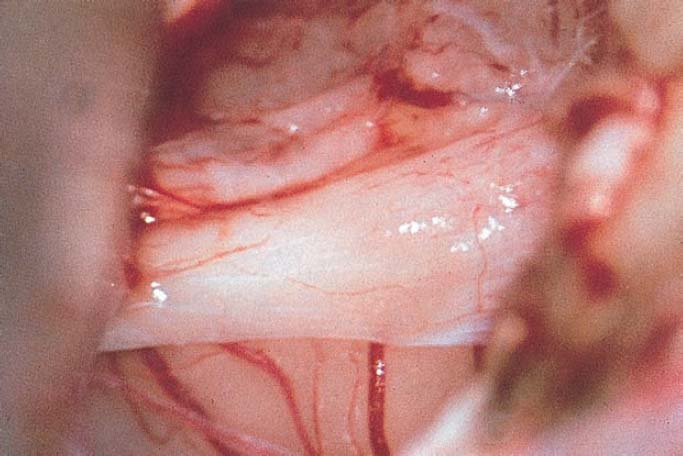
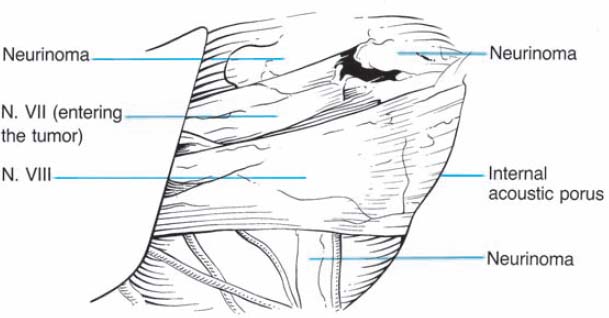
Fig. 6.1 a The cerebellopontine angle has been exposed, and a very large tumor is visualized behind the thinned-out intact eighth nerve. Notice the seventh nerve as it proceeds from the brain stem directly into the tumor.
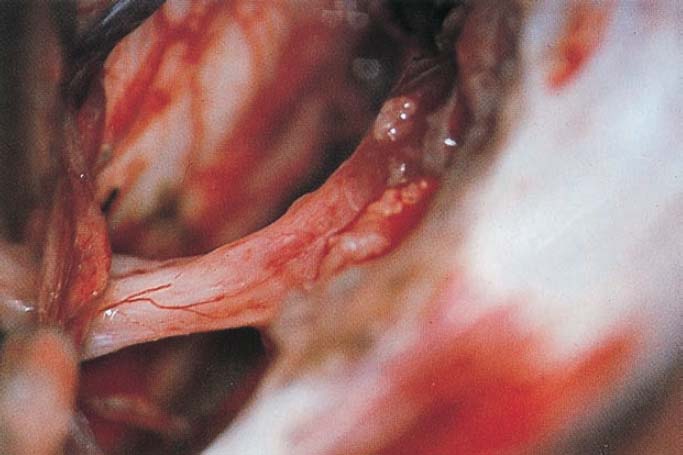
Fig. 6.1 b The tumor has been completely removed, and the eighth nerve can be visualized from the brain stem to the opened internal acoustic meatus.
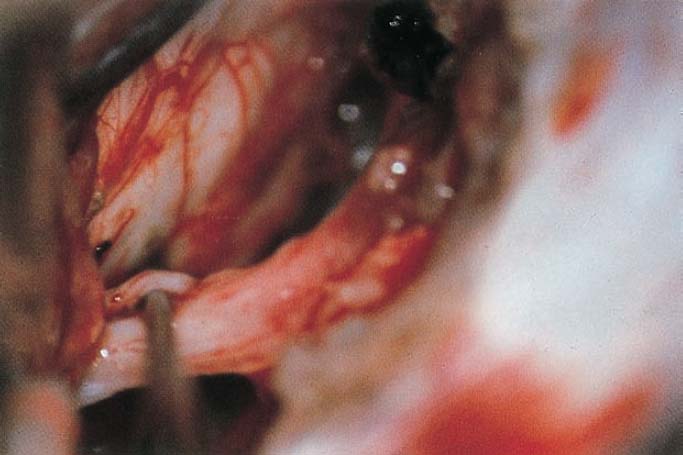
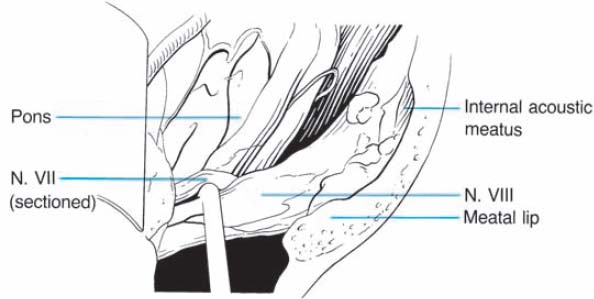
Fig. 6.1 c The stump of the facial nerve is elevated as it exits from the brain stem. This nerve was reconstructed at its distal end with an interposition nerve graft.
Case 2 (Fig. 6.2)
Diagnosis | Neurinoma of the facial nerve |
Approach | Retromastoid transmeatal |
Result | Total resection |
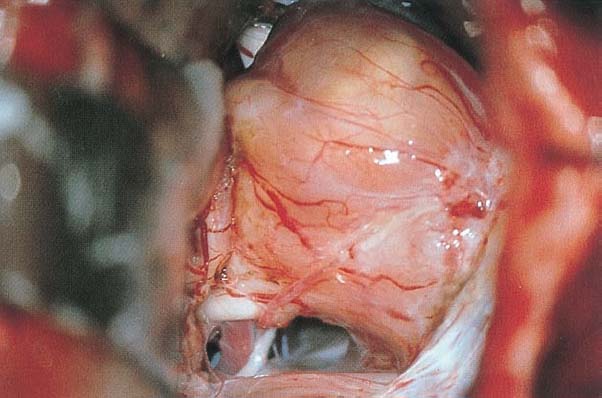
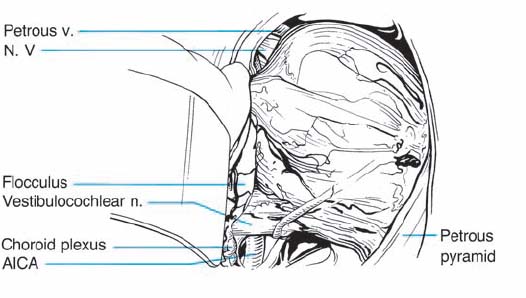
Fig. 6.2 a A large neurinoma of the facial nerve has been exposed in the right cerebellopontine angle. The uninvolved and functioning eighth nerve is visualized at the lower circumference of the tumor.
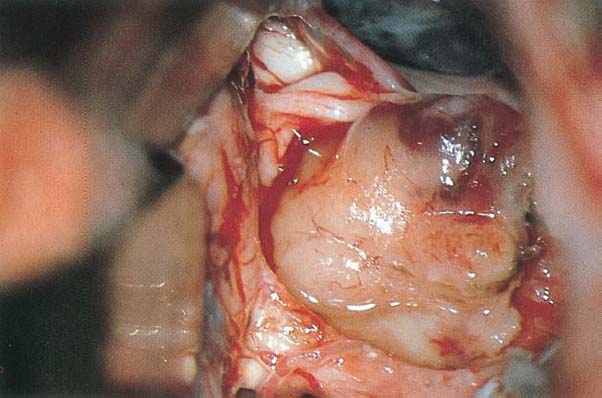
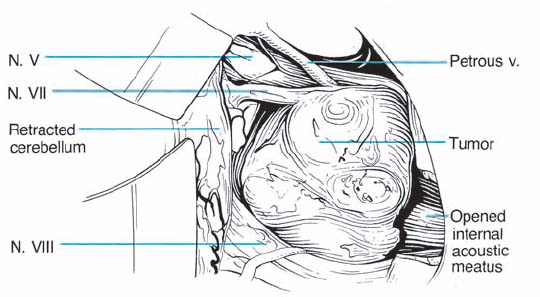
Fig. 6.2 b The neurinoma has been partially removed, and the eighth nerve is separated from the tumor capsule. A solid part of the facial nerve is visualized as it enters the upper pole of the tumor.
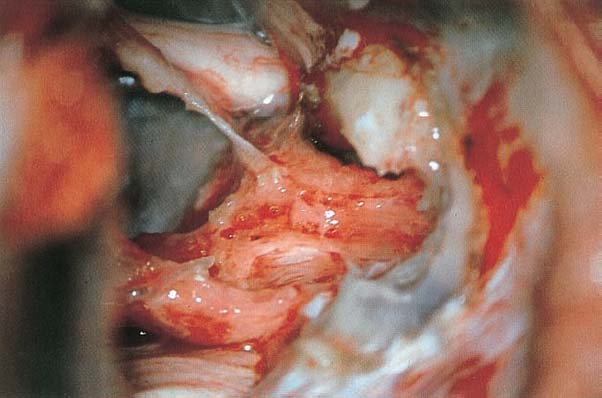
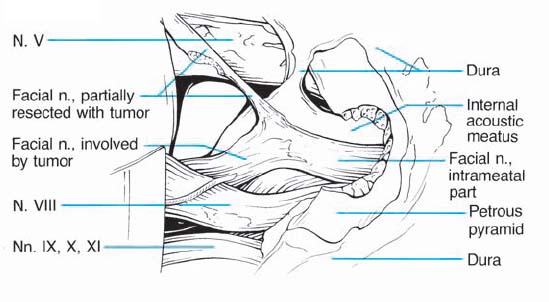
Fig. 6.2 c The situation after total resection of the intracranial and intrameatal portions of the tumor. Note the two separate parts of the facial nerve as they proceed from the brain stem to the opened internal acoustic meatus. The uninvolved portion of the seventh nerve maintains its anatomical integrity, and is displaced anteriorly. A second, separate, part of the nerve has been resected with the tumor.

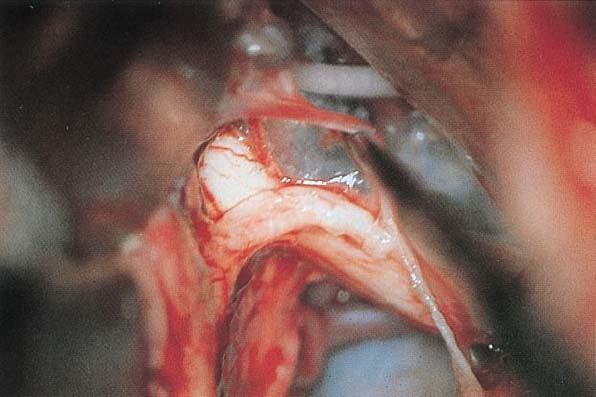
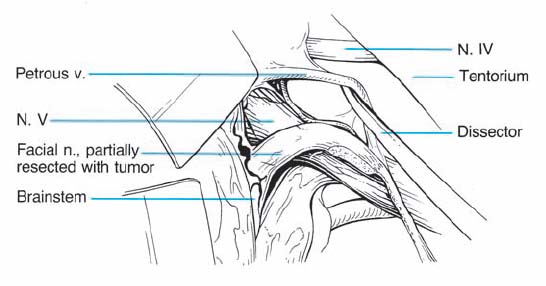
Fig. 6.2 d The microscope has been focused at the central stump of the facial nerve as it emerges from the brain stem and is displaced anterosuperiorly.
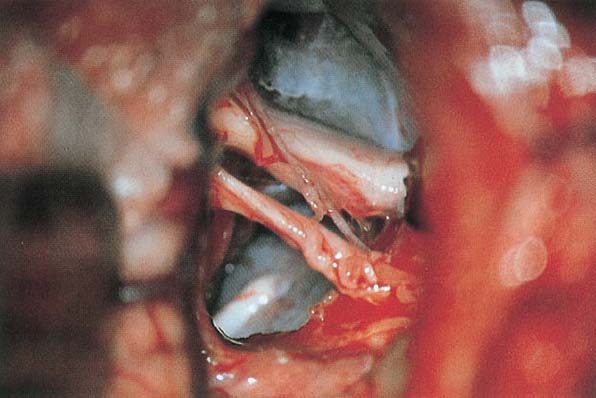
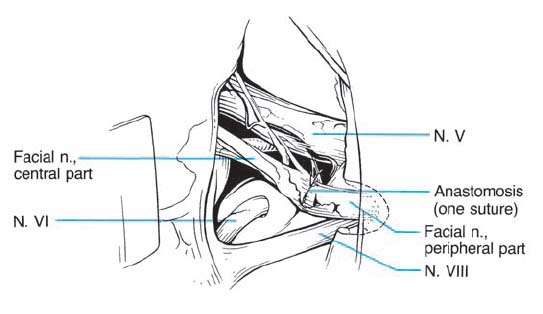
Fig. 6.2 e Note the straightened central stump of the facial nerve, anastomosed to the distal portion of the nerve using one 10–0 suture.

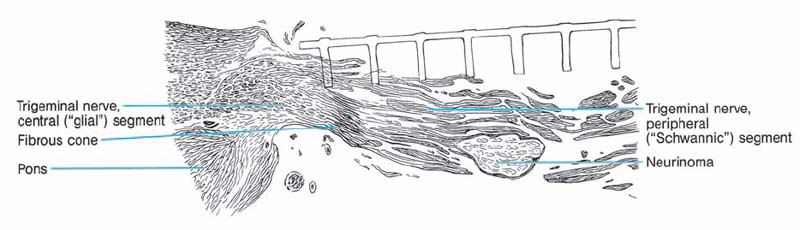
Fig. 6.3 A longitudinal section of the exit zone of the trigeminal nerve from the brain stem. There is a marked difference in color between the central (“glial”) segment and the peripheral (“schwannic”) segment of the nerve. The central nerve fibers are surrounded by glial cells, and the more peripheral fibers by Schwann cells. Note a small neurinoma growing within the peripheral segment of the sensory portion of the trigeminal nerve.
Case 2 (Fig. 6.4)
Diagnosis | Neurinoma of the trigeminal nerve |
Approach | Retromastoid transmeatal |
Result | Total resection |
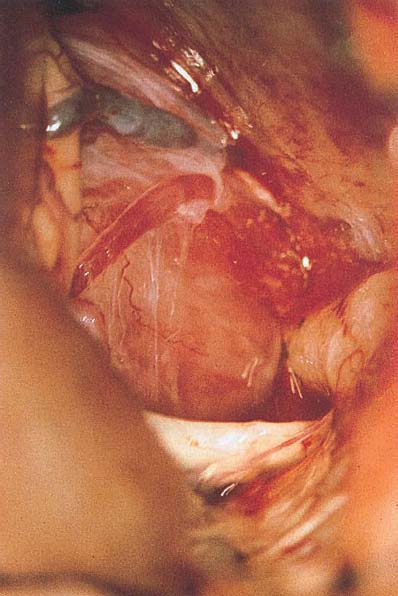
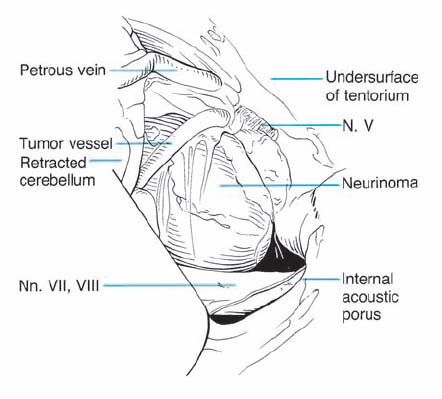
Fig. 6.4 Exposure of the superior aspect of the cerebellopontine angle reveals a large neurinoma attached to the trigeminal nerve. The most lateral intracranial portion of the trigeminal nerve is visible on the superior lateral aspect of the tumor. The seventh and eighth nerve complex can be seen coursing at the inferior aspect of the tumor. It was necessary to excise the trigeminal nerve to resect the tumor.
Neurinomas of the Glossopharyngeal Nerve
Case 1 (Fig. 6.5)
Diagnosis | Neurinoma of the glossopharyngeal nerve |
Approach | Retromastoid transmeatal |
Result | Total resection |
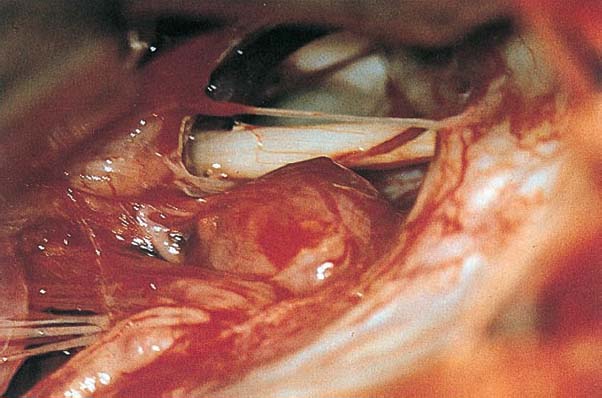
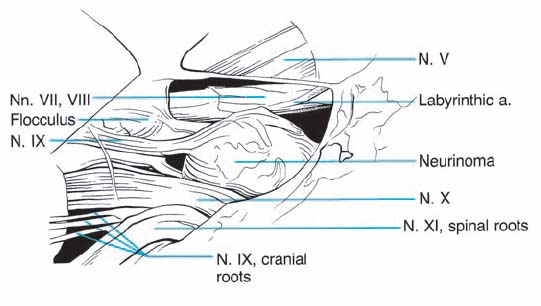
Fig. 6.5 a A view into the cerebellopontine angle reveals a tumor attached to the glossopharyngeal nerve. The seventh and eighth nerve complex can be seen above it.
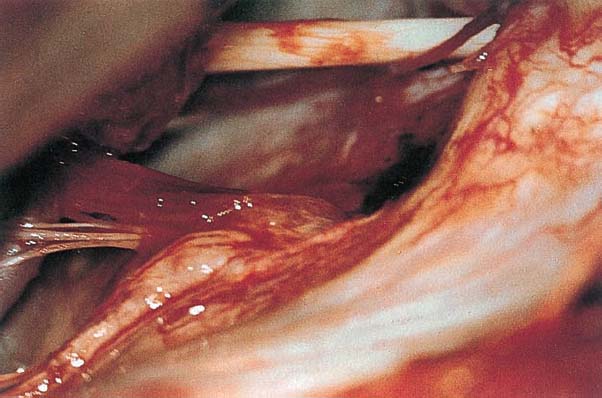
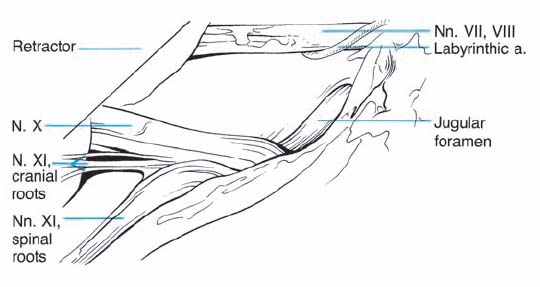
Fig. 6.5 b The tumor has been removed, and the residual glossopharyngeal nerve, the vagus filaments, and the accessory nerve are visible. The eighth nerve is seen superiorly.
Meningiomas
Case 1
F.N., male, age 42 (Fig. 6.6)
Diagnosis | Meningioma originating within the internal acoustic meatus |
Approach | Retromastoid transmeatal |
Result | Total resection, CN VII preserved, CN VIII impaired |
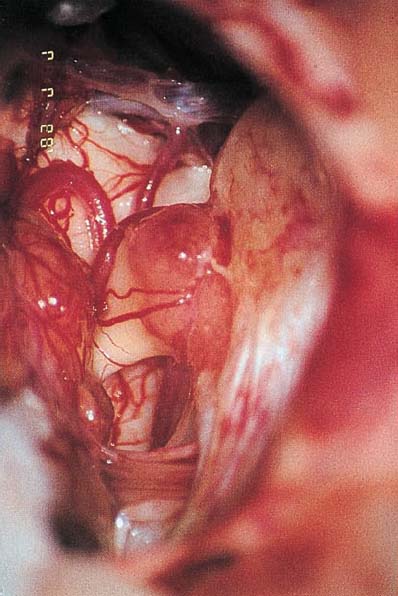
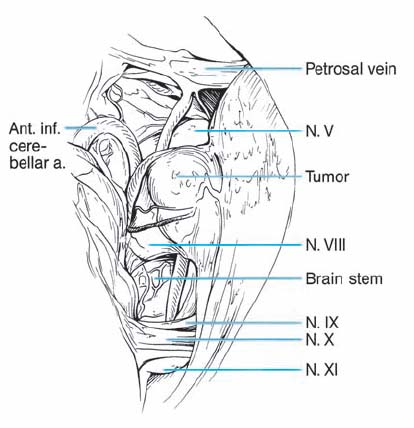
Fig. 6.6 a A small tumor in the internal auditory meatus is identified using a right retromastoid approach.
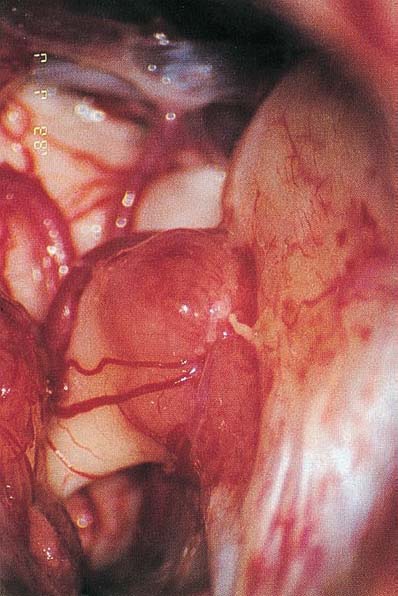
Fig. 6.6 b Higher magnification reveals the tumor as it enters the internal auditory meatus.
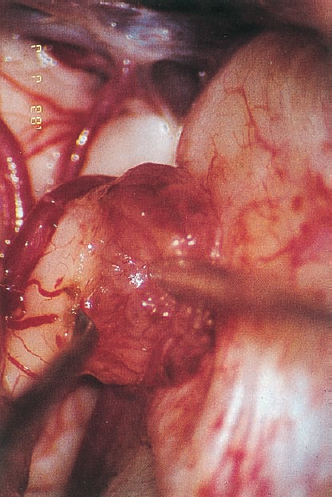
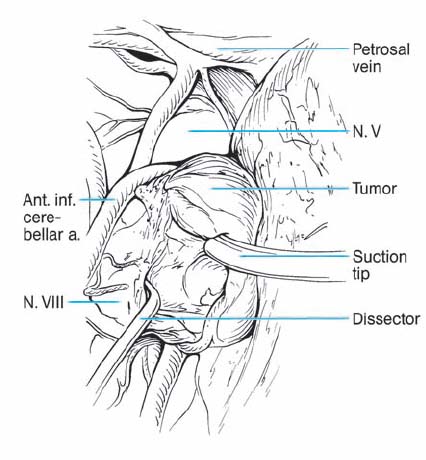
Fig. 6.6 c When the tumor is dissected from the eighth nerve complex, it is obvious that it does not involve any fascicle of the eighth nerve.
Case 2
S.N., male, age 42 (Fig. 6.7)
Diagnosis | Meningioma originating within the internal acoustic meatus |
Approach | Retromastoid transmeatal |
Result | Total resection, CN VII preserved, CN VIII preserved |

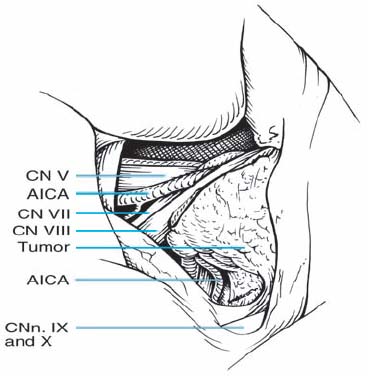
Fig. 6.7a Intraoperative exposure using a right retromastoid approach, presenting a small tumor in the region of the internal auditory meatus, similar to that in case 1. The vascularization in this case is not as typical as in the previous one. The tumor also arises more from the lower part of the meatus, lifting the cranial nerves upwards.
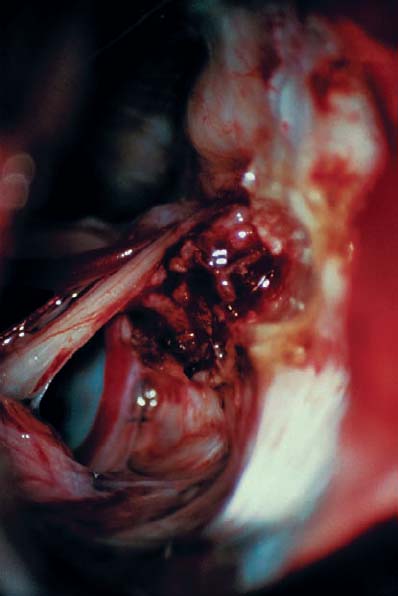
Fig. 6.7b After opening of the internal acoustic meatus, the tumor is removed in piecemeal fashion and can be identified as a meningioma.
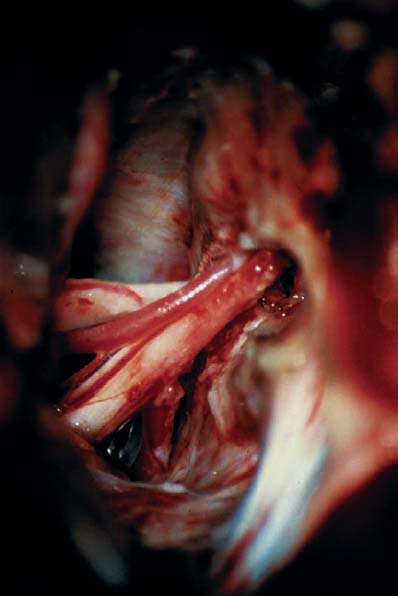
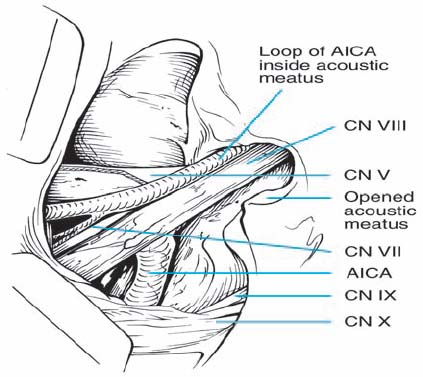
Fig. 6.7c Postoperative situation after complete tumor removal. Note the loop of the AICA and its relationship to the cranial nerves.
Case 3
Y.S., female, age 54 (Fig. 6.8)
Diagnosis | Meningioma, originating from petrous bone and tentorium |
Approach | Retromastoidal |
Result | Total resection, CN VII preserved, CN VIII preserved |

Fig. 6.8a An axial MRI scan, showing a solid mass with homogeneous contrast enhancement. The tumor originated from the posterior surface of the petrous bone. Note also that it is adherent to the upper part of the internal acoustic meatus and also to the tentorium. In this case, the lesion was identified as a meningioma. The patient had no deficits in facial or vestibulocochlear nerve function.
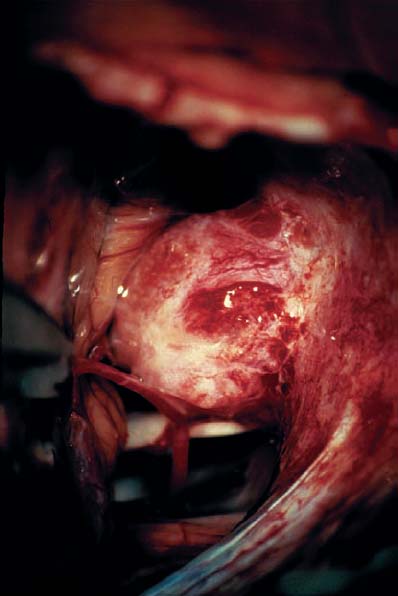
Fig. 6.8b Intraoperative exposure of the tumor in the cerebellopontine angle. The tumor itself arises from the upper part of the internal acoustic meatus, but is not invading the canal. There is a slight adhesion to the cranial nerves. Note the vascularization of this typical meningioma.
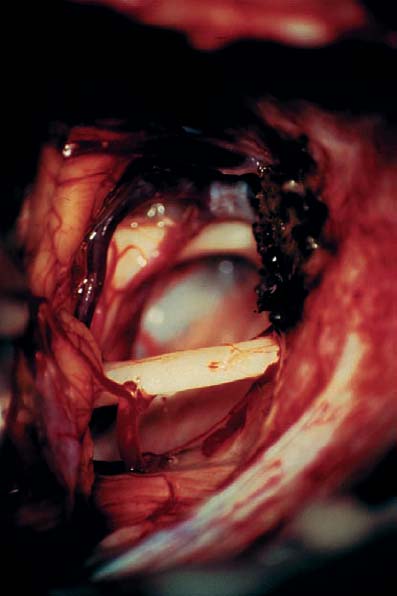
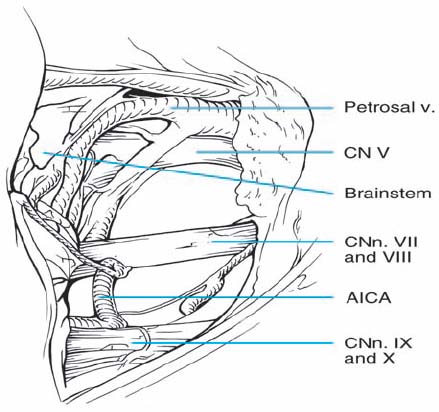
Fig. 6.8c The situation after total tumor removal, with no impairment of the cranial nerves. Note the coagulated broad appendage from the posterior part of the petrous bone.
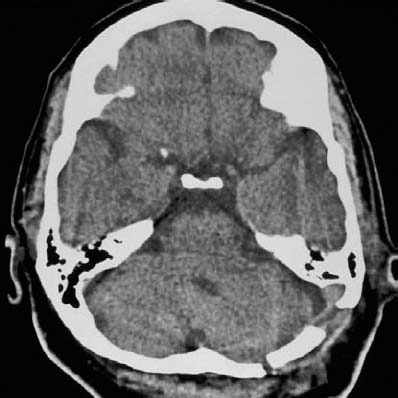
Fig. 6.8d Postoperative CT scan, demonstrating complete tumor removal. Note the surgical field and the direction of the approach. The surgery was carried out using an osteoplastic retromastoid trepanation, with the bone flap directly placed postoperatively.
Case 4
J.I., female, age 64 (Fig. 6.9)
Diagnosis | Meningioma of petrous bone and tentorium |
Approach | Retromastoidal |
Result | Total resection, CN VII preserved, CN VIII preserved |
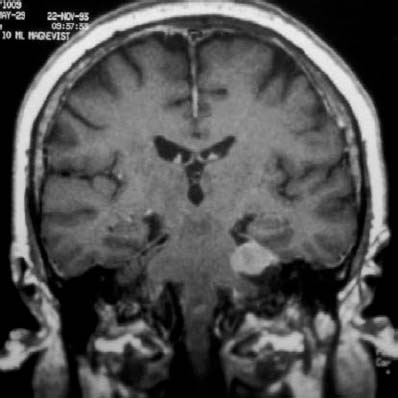
Fig. 6.9a A coronal MRI scan, showing a solid tumor with sharp boundaries, homogeneous contrast enhancement, and adhesion to the tentoriumÛtypical of a meningioma.
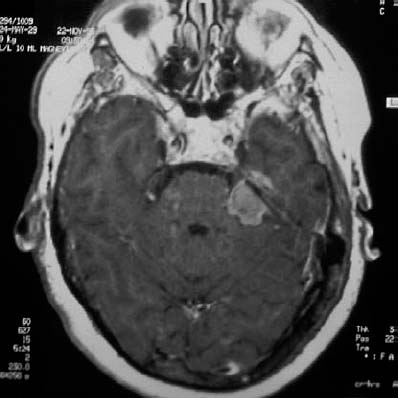
Fig. 6.9b An axial MRI scan, showing that there is also a small piece of tumor penetrating through the tentorium.

Fig. 6.9c Postoperative CT scan after total tumor removal. Note the surgical field, with no tumor remaining in place.
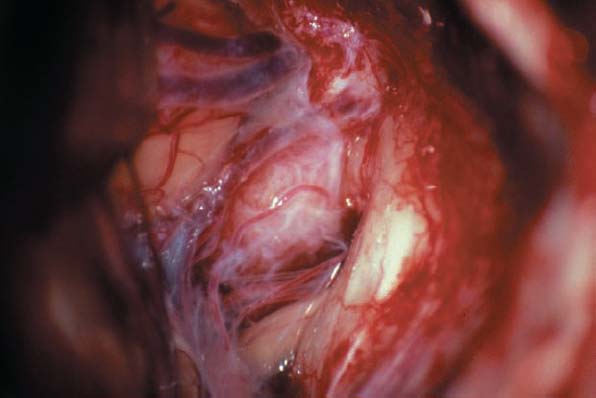
Fig. 6.9d The cerebellopontine region has been exposed, and the tumor is visualized above the cranial nerve complex, covered by arachnoid membranes.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


