Chapter 173 Overview of Imaging Procedures Available for Spinal Diagnosis
Plain-Film Radiography
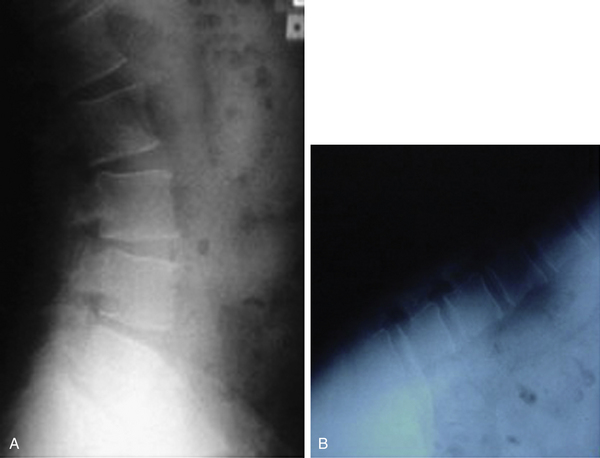
For basic anatomic depiction of the entire spinal column, plain films are optimal (Fig. 173-1). The images are relatively easy to obtain, the machines and film are readily available, and the images are mostly straightforward to interpret with a basic knowledge of spinal anatomy. Although actual hard-copy x-ray film is now replaced in many practices by direct digital images, there are still some older clinicians who insist on preserving the tactile experience of holding an x-ray film in their hands to aid in diagnosis. This will fade eventually, mostly because of cost factors (film is still fairly expensive, whereas digital images are not), but also because the benefits of going digital include the ability to change window widths, enlarge an area of interest, and store images on a central server and transmit them.1
One drawback is that proper radiographic technique must be used at all times and someone must ensure the dosages are correct and the images are diagnostic and satisfactory, or have them repeated. One must be cautious about the total ionizing radiation exposure to the patient, taking into account the number of repeated exposures endured, the part of the body being exposed, and the age of the patient.2 For instance, the total exposure of a newborn with hip dysplasia undergoing a plain radiographic examination every few weeks to determine if the therapeutic harness is working must be weighed against the fact that a superior method that does not involve ionizing radiation, ultrasonography, is available to accomplish the same end.
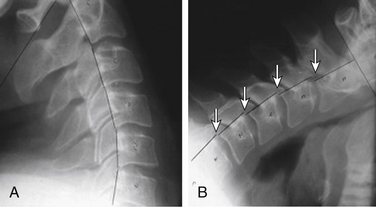
For evaluating the spine, plain radiographs have one distinct advantage over other imaging techniques: they observe the spine in a position of function, specifically, with the patient upright and bearing weight.3 This is not true of any other modality, with the exception of upright MRI (which has its own drawbacks). In addition, the spine can be imaged from a lateral viewpoint, with the patient engaging in flexion and extension, or with ventral views of the patient bending from side to side (Fig. 173-2; see Fig. 173-1). This can be performed using fluoroscopy as well, but plain radiographs are less expensive to produce and result in lower doses of radiation to the patient. Either technique is acceptable, provided the images are properly obtained and interpreted.
Plain radiographs can show excellent bony detail, assuming they are done correctly, and any fracture or misalignment is usually obvious. Instability is even more obvious if flexion and extension views are obtained.3 Congenital osseous abnormalities can be diagnosed and the normal curvatures of the spine assessed. Bearing in mind that not every individual naturally has the expected amounts of cervical and lumbar lordosis and thoracic kyphosis, observers should refrain from stating that loss of any of the spinal curvatures automatically means that the patient has muscle spasms in that region because that diagnosis can be made only by physical examination. Assessment of postural curves can be done only on upright images; otherwise, scoliosis, kyphosis, and lordosis are modified by the shape of the backboard or bed.
Myelography
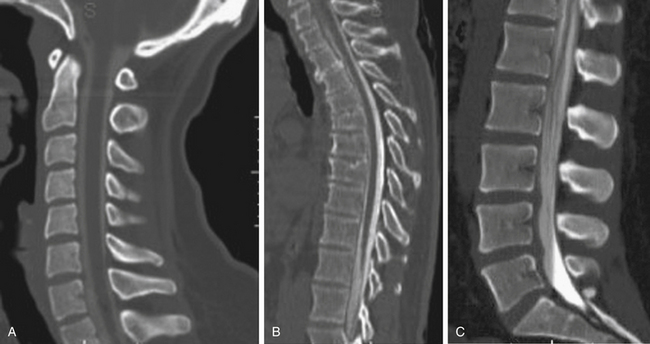
The most useful modern role of myelography is to reveal the details of the subarachnoid spaces in conjunction with anatomic detail provided by CT (Fig. 173-3). The myelogram/CT combination is the current gold standard of spinal imaging, but is used only as a last resort because it is, after all, an invasive procedure that requires a lumbar puncture and intrathecal injection.4
Fluoroscopy
This technique is essentially continuous, real-time radiography. Consequently, the dosages of radiation to the patient and to the operator can be very large if the physician is not aware of the fact that the longer the activation pedal is depressed, the more radiation is delivered.5 Although fluoroscopy can effectively evaluate motion of the spine in real time, with or without intrathecal contrast, flexion and extension plain films serve the same purpose, depict exactly the same anatomy, involve less radiation, and are less expensive to produce. The most frequent use of fluoroscopy today is in the form of the ubiquitous operating room C-arm used with every spinal surgical procedure for direction, localization, and documentation during and after surgery. It is very important that the operating physician be cognizant of the dose delivery curves for the specific machine that is being used, because they do vary according to manufacturer. Also, common sense dictates that the operator should not “keep their foot on the pedal” continually during usage, but instead develop the habit of taking “snapshots” of the target organ/structure as needed during the surgical procedure.
Computed Tomography
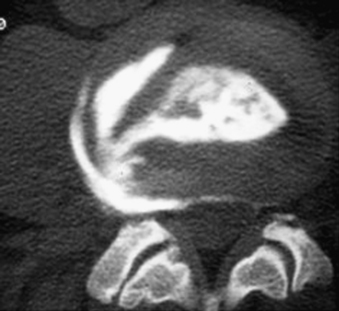
Computed tomography is an x-ray technique capable of producing images of the inside of the body using ionizing radiation (Fig. 173-4). As a result, CT carries the same risks and benefits as plain-film radiography. The x-ray source in the CT scanner is housed in a doughnut-shaped device that is capable of rotating circumferentially around the patient. Early-generation devices consisted of a single x-ray source and a single 180-degree detection device. In these devices, the x-ray beam passes through the body part of interest and exposes the detector on the opposite side in exactly the same manner as the plain radiograph is generated. Unlike plain radiographs, however, the CT x-ray source and detection device are capable of moving in tandem. After an image is created, the source and the detector move in parallel inside the cowling and another exposure is made, followed by another and then another. After the acquisition of multiple consecutive images, a computer compiles the image data and displays it according to complex algorithms as an axial image of the inside of the body part being imaged. This was a revolution—clearly as large a step forward as was Roentgen’s original hand x-ray image.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


