4
Oxygen and Gas Exchange in the Body
STEVEN H. LENIK
NOTE: This chapter corresponds to Chapter 7 in Fundamentals of Sleep Technology, 2nd edition.
RESPIRATION/VENTILATION
1. The difference between respiration and ventilation is which of the following?
A. Respiration occurs during inhalation, whereas ventilation occurs during exhalation
B. Respiration is the amount of air exchanged, and ventilation is the flow of air
C. Ventilation is mechanical gas movement; respiration is physiological gas exchange
D. Ventilation occurs during sleep, and respiration occurs while awake
GAS TRANSFER
2. The process by which oxygen enters the bloodstream from the alveoli is known as:
A. Diffusion
B. Transpiration
C. Ventilation
D. Osmosis
3. Which process removes carbon dioxide produced from cell metabolism?
A. Diffusion
B. Blood circulation
C. Ventilation
D. All of the above
OXYGEN AVAILABILITY
4. Which of the following phenomena is responsible for decreased oxygen availability at higher altitude?
A. Concentration of oxygen decreases due to less molecules.
B. Reduced temperature results in lower diffusion rate.
C. Pressure drops as the mass of air above decreases.
D. None of the above
PARTIAL PRESSURE
5. At a barometric pressure of 760 torr (or mm Hg), what is the partial pressure of oxygen in atmospheric air?
A. 21%
B. 160 torr
C. 14.7 psi
D. None of the above
OXYGEN-HEMOGLOBIN DISSOCIATION CURVE
6. Which of the following decreases hemoglobin’s ability to bind oxygen?
A. Increased CO2
B. Decreased temperature
C. Increased pH
D. Decreased hematocrit
7. Define oxygen saturation.
A. Amount of oxygen bound to hemoglobin
B. Quantity of oxygen available to the blood
C. Portion of hemoglobin’s capacity to carry oxygen
D. Percent of oxygen pressure on the hemoglobin
OXYGEN CONTENT
8. Oxygen content of the blood is determined by:
A. Total amount of hemoglobin
B. Partial pressure of oxygen (pO2)
C. Oxygen saturation (SaO2)
D. All of the above
HYPOXEMIA/HYPOXIA
9. Tissue hypoxia is caused by:
A. Low amounts of hemoglobin
B. Low partial pressure of oxygen (pO2)
C. Poor circulation
D. Poisoning
E. All of the above
CORRECTING HYPOXIA
10. The best treatment for low SaO2 in the sleep lab is:
A. Supplemental oxygen via nasal cannula
B. Continuous positive airway pressure (CPAP) to open the upper airway
C. Bilevel positive airway pressure (BPAP) with timed back-up-rate
D. None of the above
E. All of the above
EXAMPLE NO. 1: JANE DOE
11. Ms. Doe is seen in the sleep center for shortness of breath on exertion and nocturnal desaturation from an overnight oxygen saturation test. She has been observed to snore and to “hold her breath” during sleep. Polysomnography demonstrated no evidence of obstructive apneas, and only a few mild hypopneas (<5 per hour of sleep) are noted. Her baseline SaO2 is 91%, and drops to an average of 88% on falling asleep and further to 78% during REM sleep. What is the appropriate treatment?
EXAMPLE NO. 2: JOHN DOE
12. Mr. Doe presents with loud snoring, excessive daytime sleepiness and frequent dyspneic episodes, especially upon waking. Home overnight oximetry demonstrates an SaO2 nadir of 80%, and 72% of the night was spent below 90% saturation. Polysomnography shows repeated obstructive and mixed apneas and obstructive hypopneas. Baseline SaO2 is 96%, but falls to 79% during episodes of apneas. What is the appropriate treatment?
SAMPLE PROBLEM NO. 1
13. Given the data below, calculate the CaO2 and explain the data’s significance.
pO2 = 92 torr
SaO2 = 96%
Hb = 14.2 g/dL
FiO2 = 30% (or 0.30)
SAMPLE PROBLEM NO. 2
14. Given the data below, calculate the CaO2 and explain the data’s significance.
pO2 = 65 torr
SaO2 = 99%
Hb = 9.8 g/dL
FiO2 = 21% (or 0.21 or room air)
SAMPLE PROBLEM NO. 3
15. Given the data below, calculate the CaO2 and explain the data’s significance.
pO2 = 154 torr
SaO2 = 74%
Hb = 16.3 g/dL
FiO2 = 28% (or 0.28)
ANSWERS
1. C, Ventilation is mechanical gas movement; respiration is physiological gas exchange.
While ventilation refers to the movement of gas in and out of the lungs, it does not describe the process of gas exchange. Respiration is the process of oxygen and carbon dioxide exchange between the alveoli and blood, the consumption of oxygen by the tissues, and carbon dioxide production and removal from the body.
See Fundamentals of Sleep Technology, 2nd edition, Chapter 7, page 64.
Nilsson GE. Respiratory Physiology of Vertebrates. Cambridge, UK: Cambridge University Press, 2010. ISBN 978-0-521-70302-4.
Randall D. Eckert Animal Physiology. New York: W.H. Freeman and Co., 2002. ISBN 0-7167-3863-5.
Hogan MC. Respiration. In: McGinley M, Cleveland CJ, eds. Encyclopedia of Earth. Washington, DC: National Council for Science and the Environment, 2011.
2. A, Diffusion.
Gas molecules naturally travel from a region of higher pressure to one of lower pressure by the process of diffusion. Since pressure of oxygen in the alveoli is relatively higher (about 147 torr) compared to that in blood (about 50 to 70 torr), oxygen readily diffuses from the alveoli to blood. Conversely, carbon dioxide pressure in the blood is relatively higher (about 40 torr) compared to alveoli (almost 0 torr on inspiration), so carbon dioxide diffuses into the alveoli from the bloodstream.
See Fundamentals of Sleep Technology, 2nd edition, Chapter 7, page 66.
3. D, All of the above.
Tissue cells consume oxygen in order to fuel metabolic processes. Carbon dioxide (CO2) is produced as a byproduct. In order to eliminate CO2, gas is first transferred from cells to blood by diffusion. Blood carrying CO2 is pumped to the lungs by the heart (circulation and perfusion). In the lungs, CO2 is transferred from blood to the alveoli by diffusion, and finally exhaled (ventilation). The process is illustrated in Figure 4-1.
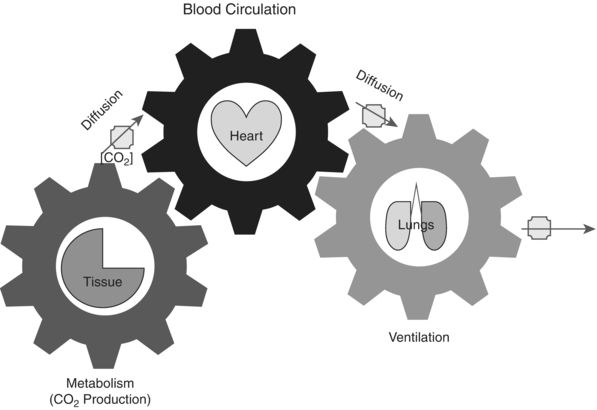
Figure 4-1 Interchange between metabolism, circulation, and ventilation.
See Fundamentals of Sleep Technology, 2nd edition, Chapter 7, page 66.
Piiper J, Dejours P, Haab P, et al. Concepts and basic quantities in gas exchange physiology. Respir Physiol. 1971;13:292–304.
Wasserman K, Whipp B, Koyal S, et al. Anaerobic threshold and respiratory gas exchange during exercise. J Appl Physiol. 1973;35:236–243.
Krogh A, Krogh M. Rate of diffusion into lungs of man. Skand Arch Physiol. 1910;23:236–247.
Crank J. The Mathematics of Diffusion. Oxford, UK: Clarendon Press, 1956.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


