Fig. 14.1
Topography of the corticospinal tract in the spinal cord. Whereas the majority of fibres cross at the level of the decussatio pyramidum, a smaller number of fibres run downward anterior paramedian near the anterior fissure and cross segmental
Two of the ascending fibre tracts whose functions are tested in every neurological examination are depicted in Fig. 14.2. All the fibres ascending in the posterior column represent axons belonging to “pseudounipolar” neurons which are located in the spinal root ganglia. This means processes leading to damage of these cells or of their axons running through the dorsal roots result in degeneration of the corresponding fibre bundles. The afferent fibres of ganglion cells form the peripheral somatic nerves. The medial part of the posterior column is named fasciculus gracilis and contains fibres from the lower body, arranged in a somatotopic fashion (Fig. 14.2). The laterally situated fasciculus cuneatus appears above T6 and is prominent in the cervical cord. The fibres of these fascicles, being thick and myelinated, convey conscious position sense, fine touch and vibratory senses.
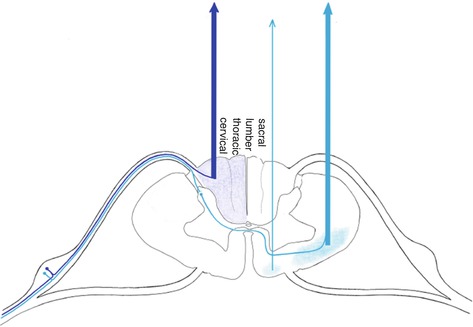
Fig. 14.2
Topography of the gracile and cuneate fascicles and the spinothalamic tracts. Whereas the fibres of the gracile and cuneate fascicles run upward ipsilateral in the dorsal columns, the fibres of the spinothalamic tracts cross segmental and run anterior and anterolateral to the brainstem
Other modalities of somatic perception, the senses of pain and temperature, are carried almost exclusively in the lateral spinothalamic tract (Fig. 14.2). Likewise, the peripheral conducting neurons are located in the spinal ganglia. However, their axons branch and connect with neurons of the posterior grey horn, running several segments up and down the spinal cord in the dorsolateral fascicle adjacent to the posterior horn (tract of Lissauer). They synapse with second-order neurons which send axons across the midline, through the anterior commissure, forming the lateral spinothalamic tract. Sensations of pressure and simple or light touch are conveyed in the ventrolateral spinothalamic tract.
The spinocerebellar tracts represent two further ascending pathways (Fig. 14.3), reaching the cerebellum via the inferior and superior cerebellar peduncles. They provide signals of unconscious position sense. This information arrives via the peripheral nervous system and, again, is transmitted via spinal root ganglia cells. However, the axons of the corresponding cells terminate on neurons of the spinal grey matter and the fibres forming the spinocerebellar tracts originate from these second-order neurons (see Chap. 16).
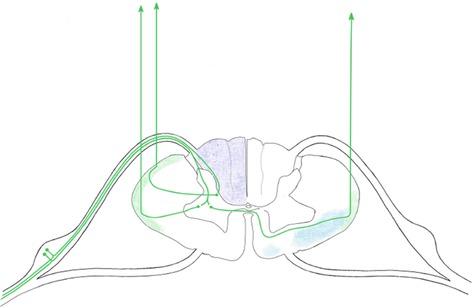
Fig. 14.3
Topography of the spinocerebellar tracts
14.3 Space-Occupying Centromedullary Lesions
Sometimes a remarkable discrepancy is to be observed between the extension of an intramedullary spinal mass and neurological deficits being minor only. This may be the case with ependymoma. When located cervically these tumours originate from the central canal, grow slowly and compress rather than infiltrate. The first and possibly only deficits result from the damage of crossing fibres of the spinothalamic tract adjacent to the central canal, leading to segmental anaesthesia of the dissociated type in the upper extremities or just below on the torso (Figs. 14.2, 14.4 and 14.5).
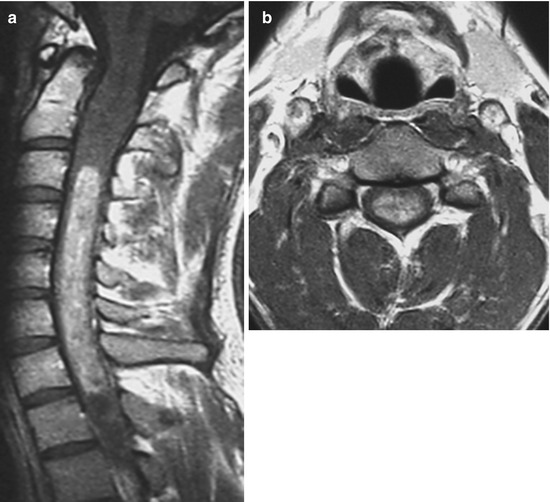
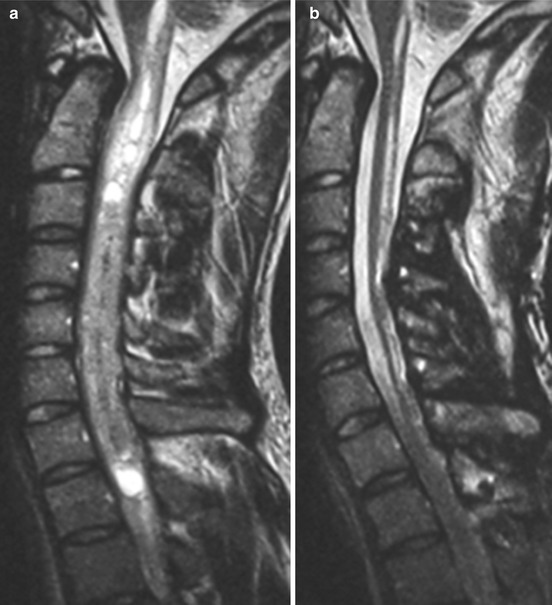
Fig. 14.4
T1 WI post contrast (pc) (a sag.; b ax.) showing an extended intramedullary space occupying lesion with relatively homogeneous enhancement, i.e. ependymoma, level C2–C7. The 25-year-old man suffered from episodic pain between the shoulders for several months and clinical examination disclosed dissociated anaesthesia in the left arm and slight proximal paresis of the upper extremities
Fig. 14.5
Preoperative sagittal T2 WI (a, b postoperative) showing a large intramedullary space occupying cervical lesion with inhomogeneous hyperintense signal changes and cystic aspects. Despite obvious atrophic changes and longitudinal hyperintense signal changes with relationship to the central canal on postoperative MRI (b), gait was possible without assistance, and bladder as well as bowel function showed no disturbances
Similarly, cavities within the spinal cord may exert pressure effects.
Hydromyelia was the term originally applied to describe regular moderate extensions of the central canal, possibly extending throughout the entire cord and communicating with the fourth ventricle. It might be viewed as a normal variation and should not be symptomatic. However, if associated anomalies are verified (for instance hydrocephalus or hindbrain malformation), further distension and deficits may result.
In the case displayed in Figs. 14.6 and 14.7), a communication of the central canal with the fourth ventricle seems unlikely. The channel is striking because it is filled with an abnormally composed fluid containing fat. Distensions not communicating with the fourth ventricle are associated with obstructions of the cerebral spinal fluid-circulation at or below the foramen magnum, spinal arachnoiditis or tethered cord (see Fig. 14.7) [3].

Fig. 14.6




First (a, b) and follow-up MRI 17 months later (c, d); sagittal T1 WI without (a, c) and with fat saturation (b, d) showing a channel filled with a fluid containing fat in a 33-year-old man
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
