Chapter 27 Patient Selection for Spine Surgery
Between 70% and 85% of all people will have back pain at some time in their lives.1 Lumbar spine disorders are the most common cause of disability in persons younger than 45 years of age.2 More than 500,000 lumbar procedures are performed each year for the treatment of lumbar spine disorders.3 Of those with low back pain (LBP), approximately 151,000 undergo a lumbar fusion each year.4 Given the large number of individuals that experience back pain, one can only surmise that the number of surgeries performed on the lumbar spine will continue to increase. The vast majority of patients with lumbar spine problems do not require surgery. Nonoperative treatment, however, is very expensive, and the data regarding its efficacy demonstrate equivocal results, at best. It is important for the physician to truly appreciate the indications for lumbar spine surgery, and also to become adept at determining the optimal surgical procedure when surgery is indeed indicated. Based on the best evidence available, this chapter addresses patient selection, clinical management results, and surgical outcomes of surgery for LBP.
Patient Evaluation
Individual factors such as work-related injuries and psychosocial support also should be assessed. Low job satisfaction, litigation, and workers’ compensation can be predictive of a poor outcome.5 Trief et al. looked at 160 patients who underwent lumbar spinal fusion. The patients completed preoperative questionnaires regarding their mental health, functional status, workers’ compensation, and job satisfaction. Patients with higher mental component scores reported less back and leg pain.5 In randomized controlled trials (RCTs) from Fairbank et al.6 and Fritzel et al.,7 patients in litigation did worse after spinal fusion than their counterparts who were not in litigation. With these studies, however, both subgroups that underwent surgery (with and without litigation) did better than the matched patients who underwent conservative management. The group of patients with the worst response overall were the patients in litigation who received conservative treatment. This, however, was not statistically significant. In another RCT by Haag et al.,8 several sociologic factors were analyzed 2 years after fusion (workers’ compensation, disability pension, unemployment, sick leave due to back pain, cohabitant/married). Overall, the operative group did better than the conservative treatment group. However, the groups that realized the greatest improvement were patients with a lighter job, not cohabiting/married, and not on sick leave. In a recent literature review, Mroz et al.9 demonstrated that people in litigation usually fare poorly. Nevertheless, they do even worse with conservative treatment. They concluded that socioeconomic factors should not be the sole factor to contraindicate surgical treatment for back pain. Health-related factors such as obesity and smoking also play a role. Recent studies have demonstrated an increase in surgical site infections in morbidly obese patients.10 Elderly obese patients undergoing lumbar surgery report a high rate of dissatisfaction with the surgery outcome compared with nonobese patients.10 Smoking is known to be a predictor of poor surgical outcome in lumbar fusion surgery. Habitual nicotine use is thought to decrease the revascularization of the graft, slowing healing rates and increasing the risk of infection and of pseudarthrosis.11 There are no clear guidelines on preoperative lumbar fusion and cessation of smoking. However, patients should be encouraged to stop smoking as early as possible before undergoing surgery to increase the chance of long-term success.
Chronic LBP may trigger anxiety, depression, and fear, thereby changing the way people perceive pain. The Minnesota Multiphasic Personality Inventory (MMPI) is one of the most widely used personality tests. Patients are asked to answer questions regarding their anxiety and depressive symptoms. The scale attempts to identify patients who are preoccupied with their symptoms, are depressed, or feel a high level of anxiety, because these individuals tend to fare worse.12 These factors are more predictive of a good outcome than physical findings or radiographic measures. Studies have suggested that fear-avoidance beliefs about physical activity and work might form specific cognitions intervening between LBP and disability.13 A Fear-Avoidance Beliefs Questionnaire (FABQ) was developed, based on theories of fear and avoidance behavior and focused specifically on patients’ beliefs about how physical activity and work affected their LBP. FABQ screening could be useful in patient evaluation for lumbar surgery because it could accurately identify subjects with elevated levels of fear.13
After the history is collected, the physical examination should focus on deficits in sensation, muscular weakness, deep tendon reflexes, and any abnormal reflexes such as a Hoffman or Babinski reflex.14 The clinician also should be aware of any suspicious symptoms or signs that are consistent with malingering. These physical examination findings include pain at the top of the tailbone, entire leg pain or numbness, giveaway weakness, persistent pain, intolerance to treatment, and multiple emergency admissions to hospitals with simple backache (Waddell signs). Clinicians should also be wary of patients who present with a gross limp, use of physical supports (e.g., corset, crutches, transcutaneous electrical nerve stimulation [TENS] unit), or any continuous or repetitive movement.15 A well-performed hip examination that includes palpation of the greater trochanter to rule out bursitis as well as rotational maneuvers to rule out primary hip joint pathology is imperative when examining the lumbar spine, as are the shoulder and upper extremity peripheral nerves examination when examining the neck. It is very important to be aware of and not miss the “red flag” signs in a patient with pain of spinal origin. The clinician should consider ordering imaging studies after the first encounter in patients with a history of trauma, night pain, weight loss, cancer, persistent weakness, urinary or fecal incontinence, saddle anesthesia, or constitutional symptoms.16
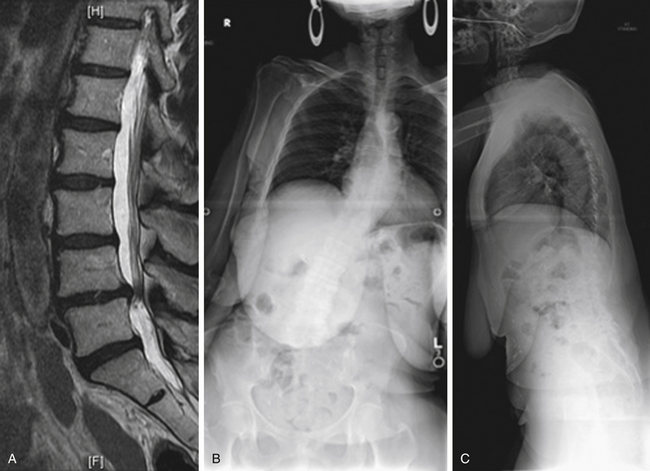
Case Presentation 1: The Importance of Standing Films
The patient presented with a chief complaint of L3, L4, and L5 radiculopathy in the right lower extremity. The MRI examination (Fig. 27-1A) shows stenosis, predominantly foraminal (not shown in this cut). No deformity or instability is observed. On standing radiographs (Figs. 27-1B and C), 12-cm coronal and 17-cm sagittal imbalances are discovered. The imbalances significantly affect the clinical decision-making process.
Low Back Pain: Evidence for Treatment
Low Back Surgery for Adult Low-Grade Spondylolisthesis
Conservative versus Surgical Treatment
Two RCTs,18 (same population, different follow-up) comparing low-grade spondylolisthesis patients with those who presented with either chronic LBP or radiculopathy, or both, treated either with fusion or conservative treatment, found that the surgical group did statistically and clinically better, as assessed by pain scores and the Disability Rating Index (DRI). Even though the long-term follow-up (5 years) showed that some of the initial improvement (1–2 years) had been lost, 76% of the patients in the surgical group still considered their overall outcome as “much better” compared with only 50% in the conservative group. Another prospective RCT found significant difference when treating patients with low-grade spondylolisthesis with an advanced core strengthening program performed by a specialist physical therapist and a control group that performed simple exercises prescribed by their primary physician at 3, 6, and 30 months. The advanced exercise group had better outcomes.19 Sinaki et al. have shown, in a retrospective analysis, significant benefit of flexion exercises in comparison with extension exercises to control the symptoms of low-grade spondylolisthesis.20 Daniel et al. reported very poor results with conservative treatment for spondylosis, including the use of a full-time thoracolumbar orthosis. Twenty-nine of 31 patients failed treatment and progressed to surgery.21
Low-Grade Spondylolisthesis: To Fuse or Not to Fuse? Role of Instrumentation? Best Approach?
When assessing the role of fusion in the management of adult low-grade spondylolisthesis, Herkowitz and Kurz22 performed an RCT comparing decompression alone with decompression and uninstrumented PLF (posterolateral fusion). A mean 3-year follow-up demonstrated better outcomes for leg and back pain for the fusion group (P = .0001). Other authors in prospective nonrandomized23 and retrospective24–26 series also support decompression and fusion over decompression alone when spondylolisthesis is present.
The role of instrumentation in achieving fusion and improving clinical outcomes in low-grade spondylolisthesis was studied by Fischgrund et al.27 in an RCT. Patients were divided into two groups: (1) decompression and noninstrumented PLF and (2) decompression with instrumented PLF (pedicle screws). The fusion rate was 83% versus 45%, respectively, for the instrumented versus noninstrumented groups. Clinical outcomes, however, were similar for both groups (78% vs. 85%, instrumented vs. noninstrumented). Kornblum et al. 28 combined the noninstrumented patients from both the Fischgrund27 and the Herkowitz22 studies to compare 47 patients with either a solid fusion or a nonunion. The solid fusion group had a satisfactory result in 86% of patients, whereas patients in the nonunion group had 56% satisfactory results at 5 to 14 years of follow-up.
Two additional RCTs were performed. In these studies, instrumentation was associated with higher fusion rates and better clinical outcomes for low-grade spondylolisthesis. Zdeblick29 reported a 65% fusion rate and 71% satisfactory clinical outcome in the noninstrumented group, versus a 95% fusion rate and 95% satisfactory clinical outcome in the rigid instrumentation group. Bridwell et al.30 randomized 43 patients into three groups: (1) decompression only, (2) decompression with uninstrumented posterolateral fusion, and (3) decompression with rigid pedicle screw instrumentation posterolateral fusion. The fusion rates were 33% and 87.5% for groups 2 and 3. Clinical improvement was 30%, 33%, and 83.3% for groups 1, 2, and 3, respectively.
Kwon et al.31 reviewed the literature regarding surgical approaches to low-grade spondylolisthesis (ventral/dorsal/360 degrees). In a total of 1100 patients from 34 studies (4 of which were RCTs), the clinical results and fusion rates were better when the combined ventral/dorsal approach was used. When comparing anterior lumbar interbody fusion (ALIF) plus PLF with instrumentation versus ALIF plus instrumentation without PLF, Shofferman et al.32 found that both groups had improvement in function, but no difference in results could be detected.
In 2005, the Scoliosis Research Society released a consensus statement on the treatment of low-grade acquired/isthmic spondylolisthesis,33 making the following points:
• The achievement of a solid fusion is associated with better clinical outcomes.
• The adjunctive use of pedicle screw instrumentation improves fusion rates.
• While instrumentation does not show significant improvement on patient-scored outcome measures, the positive effect on fusion alone warrants its use.
• There is no consensus regarding the approach for fusion—interbody, dorsolateral, or combined.
Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Medical Management of Adult and Pediatric Spinal Cord Injury
Cervical Skip Corpectomy
Percutaneous and Minimally Invasive Approaches to Decompression and Arthrodesis of the Thoracolumbar Spine
Medical Management of the Patient with Acute Spinal Cord Injury
Spine Infection
Definition and Assessment of Dysfunctional Segmental Motion
Medical Management of Adult and Pediatric Spinal Cord Injury
Cervical Skip Corpectomy
Percutaneous and Minimally Invasive Approaches to Decompression and Arthrodesis of the Thoracolumbar Spine
Medical Management of the Patient with Acute Spinal Cord Injury
Spine Infection
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


