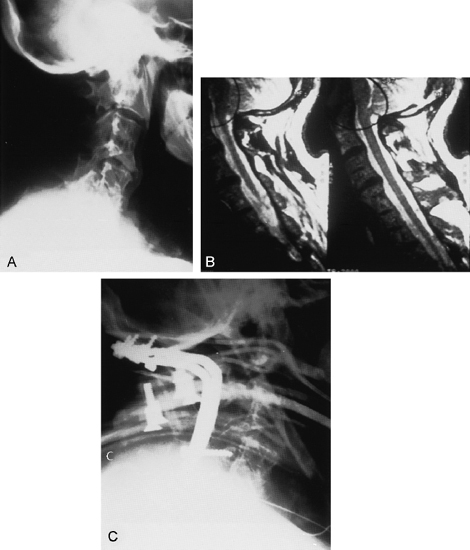
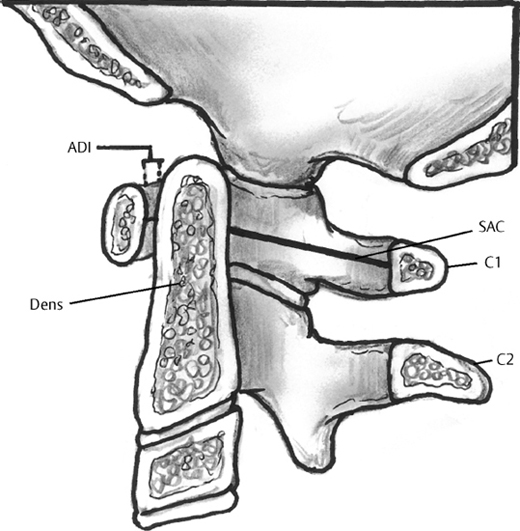
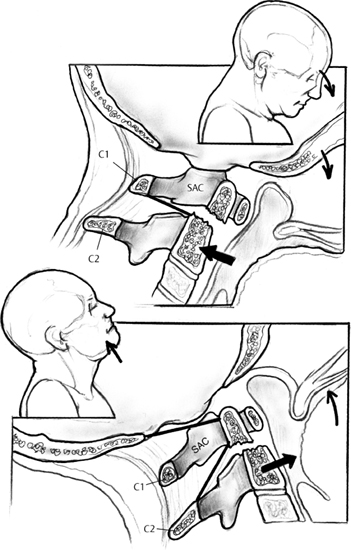
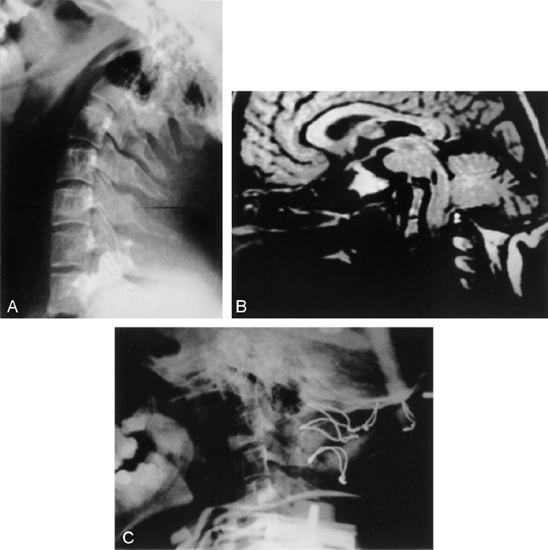
23 I. Developmental anatomy A. Atlas 1. Neurocentral synchondrosis forms at 6 to 24 months. a. Fusion begins at 4 to 6 years. b. Posterior synchondrosis fuses at 5 years. B. Dens 1. Two primary ossification centers coalesce at 1 to 3 months of age. 2. Separated from the vertebral body by a dentocentral synchondrosis that fuses at 6 to 8 years C. Normal variants 1. Posterior bifid C1 arch 2. Bipartite superior articular surface of the atlas 3. Pseudonotch of the atlas 4. Absence or partial absence of the posterior arch of the atlas 5. Posteriorly displaced spinolaminar line of the axis 6. Posteriorly angulated dens 7. Pseudosubluxation of the axis (less than 10 years old) II. Physical examination A Limited range of motion B. Torticollis C. Facial asymmetry D. Associated abnormalities 1. Scoliosis, renal, cardiac, or other head and neck anomalies III. Radiographic evaluation (Figs. 23–1, 23–2) A. Flexion-extension view is very important to assess stability. B. Critical measurements on flexed lateral view 1. Atlantoaxial interval: 4.5 mm (children), compared with 3 mm (adults) 2. Space available for spinal cord (SAC): 13 mm IV. Specific disorders A. Basilar invagination (Fig. 23–3) 1. Deformity of the bones at the base of the skull at the margin of the foramen magnum a. The odontoid is migrated cephalad. 2. Types a. Primary (1) Congenital (2) Associated with other findings (a) Atlanto-occipital fusion (b) Hypoplasia of atlas (c) Bifid posterior arch of the atlas (d) Odontoid abnormalities (e) Klippel-Feil syndrome b. Secondary (1) Developmental condition with softening of the base of the skull (2) Associated with other clinical disorders (a) Osteomalacia (b) Rickets (c) Paget’s disease (d) Osteogenesis imperfecta (e) Renal osteodystrophy (f) Rheumatoid arthritis (g) Neurofibromatosis (h) Ankylosing spondylitis (i) Achondroplasia 3. Clinical findings a. Commonly become symptomatic in second and third decades (1) Short neck (2) Asymmetric face (4) Weakness/paresthesias (5) Cranial nerve palsies (6) Cerebellar signs (unsteady gait and nystagmus) (7) Pain (head and neck) (8) Syncope and dizziness (vertebral artery compression) (9) Seizures/hydrocephalus (cerebrospinal obstruction) 4. Treatment a. Posterior impingement (1) Suboccipital craniectomy and decompression of the posterior ring of C1 with posterior stabilization b. Anterior impingement (1) Mobile odontoid (a) Occipitocervical fusion in extension is recommended (2) If the odontoid cannot be reduced, anterior excision of odontoid and posterior stabilization is recommended. B. Klippel-Feil syndrome (Fig. 23–4) 1. Congenital fusion of cervical vertebrae 2. Failure of normal segmentation of cervical spine during the third to eighth week 3. Associated anomalies a. Genitourinary (35%) b. Central nervous system c. Cardiopulmonary d. Sprengel’s deformities (40%) e. Upper extremity anomalies f. Scoliosis (60%) 4. Clinical findings a. Low posterior neck line b. Short neck c. Limited neck motion (1) Majority have normal appearance with mild restriction of motion. 5. Radiographic findings a. Vertebral synostoses b. Flattening and widening of the vertebral bodies c. Absent disc spaces or hypoplasia 6. Treatment a. The majority of patients are asymptomatic. (1) Symptoms may appear later in life. b. Conservative treatment is indicated for most patients. (1) Anti-inflammatory medications (2) Exercise program c. Fusion may be indicated in select patients with instability and spinal cord impingement. C. Anomalies of the odontoid 1. Etiology a. Trauma (1) Salter I fracture with a nonunion
Pediatric Cervical Spine Disorders
Neupsy Key
Fastest Neupsy Insight Engine