Chapter 5 Peripheral Nerve Disorders
Anatomy
The spinal cord’s anterior horn cells form the motor neurons of the peripheral nerves – the PNS’ starting point. The peripheral nerves are the final link in the neuron chain that transmits motor commands from the brain through the spinal cord to muscles (Fig. 5-1). Nerve roots emerging from the anterior spinal cord mingle within the brachial or lumbosacral plexus to form the major peripheral nerves, such as the radial and femoral. Although peripheral nerves are quite long, especially in the legs, they faithfully conduct electrochemical impulses over considerable distances. Because myelin, the lipid-based sheath generated by Schwann cells, surrounds peripheral nerves and acts as insulation, the impulses are preserved.
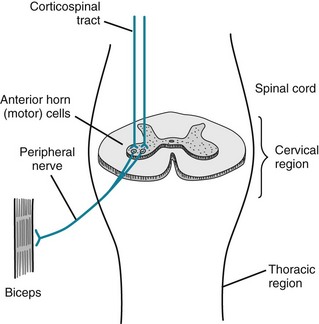
FIGURE 5-1 The corticospinal tracts, as discussed in Chapter 2, and as their name indicates, consist of upper motor neurons (UMNs) that travel from the motor cortex to the spinal cord. They synapse on the spinal cord’s anterior horn cells, which give rise to the lower motor neurons (LMNs). The LMNs join sensory fibers to form peripheral nerves.
When stimulated, motor nerves release packets of acetylcholine (ACh) from storage vesicles at the neuromuscular junction. The ACh packets traverse the junction and bind on to specific ACh receptors on the muscle end plate. The interaction between ACh and its receptors depolarizes the muscle membrane and initiates a muscle contraction (see Chapter 6). Neuromuscular transmission culminating in muscle depolarization is a discrete, quantitative action: ACh does not merely seep out of the presynaptic terminal as loose molecules and drift across the neuromuscular junction to trigger a muscle contraction.
Mononeuropathies
Disorders of single peripheral nerves, mononeuropathies, are characterized by flaccid paresis, DTR loss (areflexia), and reduced sensation, particularly for pain (hypalgesia [Greek, hypo, under + algos, pain] or analgesia [Greek, insensitivity to pain]) (Table 5-1). Paradoxically, mononeuropathies and other peripheral nerve injuries sometimes lead to spontaneously occurring sensations, paresthesias (Greek para, near + aisthesis, sensation) that may be painful, dysesthesias. Peripheral nerve injuries also convert stimuli that ordinarily do not cause pain, such as a light touch or cool air, into painful sensations, allodynia; exaggerate painful responses to mildly noxious stimuli, such as the point of a pin, hyperalgesia; or delay but then exaggerate and prolong pain from noxious stimuli, hyperpathia.
TABLE 5-1 Major Mononeuropathies
*Compression of the radial nerve in the spiral groove of the humerus spares the triceps deep tendon reflex (DTR).
Compression, especially of nerves protected only by overlying skin and subcutaneous tissue rather than by bone, viscera, or thick layers of fat, occurs frequently. People most susceptible are diabetics; those who have rapidly lost weight, thereby depleting nerves’ protective myelin covering; workers in certain occupations, such as watchmakers; and those who have remained in disjointed positions for long periods, often because of drug or alcohol abuse. One of the most common compressive mononeuropathies – “Saturday night palsy” – affects the radial nerve, which is vulnerable at the point where it winds around in the spiral groove of the humerus. Thus, people in alcohol-induced stupor who lean against their upper arm for several hours are apt to develop a wrist drop (Fig. 5-2). Foot drop, its lower-extremity counterpart, often results from common fibular nerve* damage from prolonged leg crossing compressing the nerve, lower-knee injuries traumatizing the nerve, or a constrictive lower-leg cast pushing against the nerve as it winds around the head of the fibula.

FIGURE 5-2 As the radial nerve winds around the humerus, it is vulnerable to compression and other forms of trauma. Radial nerve damage leads to the readily recognizable wrist drop that results from paresis of the extensor muscles of the wrist, finger, and thumb.
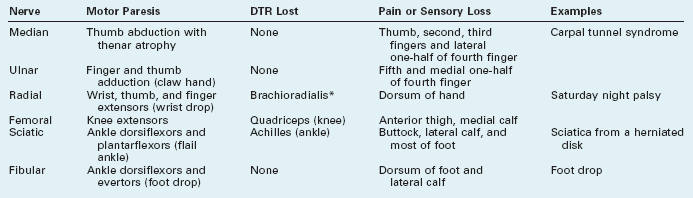
Carpal tunnel syndrome, the most common mononeuropathy, results from damage of the median nerve as it travels through the carpal tunnel of the wrist (Fig. 5-3, left). Forceful and repetitive wrist movements can traumatize the nerve in that confined passage. Meat and fish processing, certain assembly-line work, and carpentry are all closely associated with carpal tunnel syndrome; however, contrary to initial claims, word processing and other keyboarding actually have a weak association with the disorder. In another mechanism, fluid retention during pregnancy or menses entraps the median nerve in the carpal tunnel. Similarly, inflammatory tissue changes in the wrist from rheumatoid arthritis may compress the median nerve.
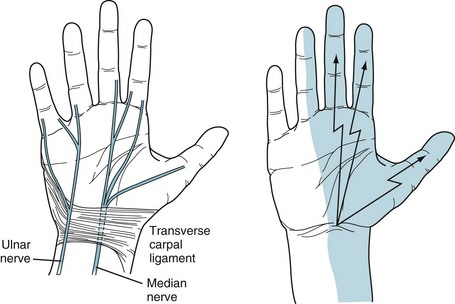
FIGURE 5-3 Left, The median nerve passes through the carpal tunnel, which is a relatively tight compartment. In it, the median nerve is vulnerable to repetitive movement and compression from fluid accumulation. The ulnar nerve, taking a different route, passes above and medial to the roof of the tunnel, the transverse carpal ligament. It thus escapes damage from most repetitive movements and fluid accumulation. Right, The usual sensory distribution of the median nerve encompasses the palm, thenar eminence (thumb base), thumb, and adjacent two fingers. In carpal tunnel syndrome, pain shoots distally from the wrist over this area. Physicians may elicit the Tinel sign, a reliable indication of carpal tunnel syndrome, by tapping the patient’s palmar wrist surface and finding that paresthesias emanate from the wrist and radiate in the median nerve distribution.
Whatever the mechanism, carpal tunnel syndrome causes paresthesias and pains that shoot from the wrist to the palm, thumb, and adjacent two or sometimes three fingers (Fig. 5-3, right). Symptoms worsen at night and awaken the victims, who shake their hands in an attempt to find relief. Neurologists test for the syndrome’s characteristic Tinel sign by percussing the wrist: The test is positive when the percussion generates electric sensations that shoot from the wrist into the palm and fingers.
In another example of upper-extremity nerve damage, pressure on the ulnar groove of the elbow (the “funny bone”) or cubital tunnel may damage the ulnar nerve. For instance, when individuals rest the weight of their arms on their elbows, the compression often injures the ulnar nerve. These individuals develop atrophy and weakness of their hand muscles (Fig. 5-4). The ulnar nerve damage also leads to loss of sensation of the fourth and fifth fingers and the medial surface of the hand.
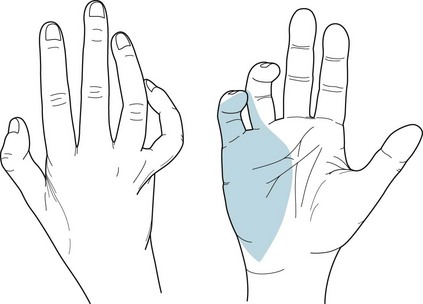
FIGURE 5-4 Left, With ulnar nerve injuries, the palmar view shows that intrinsic muscles of the hand, particularly those of the hypothenar eminence (fifth finger base), undergo atrophy. The fourth and fifth fingers are flexed and abducted. When raised, the hand and fingers assume the benediction sign. In addition, the medial two fingers and palm are anesthetic (numb). Right, Ulnar nerve injuries also produce a claw hand because of atrophy of the muscles between the thumb and adjacent finger (first dorsal interosseous and adductor pollicis), as well as of those of the hypothenar eminence.
Polyneuropathies (Neuropathies)
Alternatively, neurologists divide neuropathies into sensory, motor, or mixed sensorimotor neuropathy. Patients with sensory neuropathy usually suffer predominantly or exclusively from numbness, paresthesias, or burning in their fingers and toes (i.e., stocking-glove hypalgesia: Fig. 5-5). The pain may reach intolerable proportions (see neuropathic pain, Chapter 14). When sensory neuropathy affects the feet, it may provoke leg movements, such as restless legs syndrome (see Chapter 17). Patients with motor neuropathy usually have distal limb weakness that impairs fine, skilled hand and finger movements, such as buttoning a shirt, or raising their feet when they walk, which causes a foot drop. Their neuropathy in chronic cases usually also leads to muscle atrophy and flaccidity. As with other LMN injuries, it diminishes DTRs (see Fig. 2-2C), first at the brachioradialis and Achilles’ and then at more proximal sites. Mixed sensorimotor neuropathy causes mixtures of those symptoms and signs.
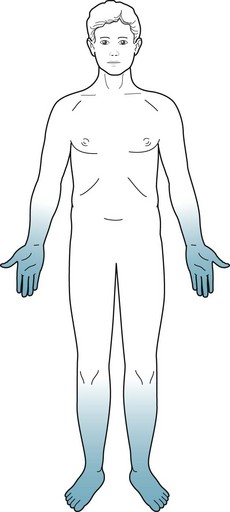
FIGURE 5-5 Patients with polyneuropathy lose pain and other sensations. The loss is symmetric, more severe distally than proximally, and more severe in the legs than arms. Neurologists term this pattern of sensory loss stocking-glove hypalgesia.
Neurologists who care for psychiatric patients may meaningfully divide neuropathies into those with and those without comorbid changes in mental status (Box 5-1).
Box 5-1
Important Causes of Neuropathy
Neuropathies Without Comorbid Mental Status Changes
Guillain–Barré Syndrome
When first affected, young and middle-aged adults feel paresthesias and numbness in the fingers and toes. Then they develop flaccid paresis of their feet and legs with characteristically absent knee and ankle DTRs. Weakness and areflexia, which soon become a much greater problem than numbness, ascend to involve the hands and arms. Many patients progress to respiratory insufficiency because of involvement of the phrenic and intercostal nerves, and require intubation for ventilation. If weakness ascends still further, patients develop cranial nerve involvement that may lead to dysphagia and other aspects of bulbar palsy (see Chapter 4). Additional involvement causes facial weakness and then sometimes even ocular immobility. Nevertheless, possibly because optic and acoustic nerves are protected by myelin generated by the CNS – not the PNS – patients continue to see and hear.
Even if the illness worsens to the point of total paralysis, patients usually remain conscious with a normal mental status – allowing for anxiety and depressive symptoms from enduring a life-threatening illness. Completely immobile and anarthric Guillain–Barré syndrome patients, typically with preserved consciousness and mental status, exist in a locked-in syndrome (see Chapter 11). Cerebrospinal fluid (CSF) exhibits an elevated protein concentration but with few white cells (i.e., the classic albumino-cytologic dissociation) (see Table 20-1).
The illness usually resolves almost completely within 3 months as the PNS myelin is regenerated. By way of treatment, plasmapheresis (plasma exchange), which extracts circulating inflammatory mediators, particularly autoantibodies, complement, and cytokines, reduces the severity and duration of the paresis. Alternatively, administration of intravenous human immunoglobulin, which “blocks” the antibodies at the neuromuscular junction, also restores patients’ strength. Steroids will not help, which is surprising because they are helpful in other inflammatory diseases of the nervous system, such as myasthenia gravis (see Chapter 6), multiple sclerosis (MS: see Chapter 15), and the chronic form of Guillain–Barré syndrome (chronic inflammatory demyelinating polyneuropathy).
Not only is Guillain–Barré syndrome a life-threatening illness, but it also epitomizes the distinction between PNS and CNS diseases. Although paraparesis or quadriparesis might be a feature common to PNS and CNS illnesses, different patterns of muscle weakness, changes in reflexes, and sensory distribution characterize PNS and CNS illnesses (Table 5-2). Also, in Guillain–Barré syndrome, as in most neuropathies other than diabetic neuropathy (see later), bladder, bowel, and sexual functions are preserved. In contrast, patients with spinal cord disease usually have incontinence and impotence at the onset of the injury.
TABLE 5-2 Differences between Central (CNS) and Peripheral Nervous System (PNS) Signs
| CNS | PNS | |
|---|---|---|
| Motor System | Upper motor neuron | Lower motor neuron |
| Paresis | Patterns* | Distal |
| Tone | Spastic† | Flaccid |
| Bulk | Normal | Atrophic |
| Fasciculations | No | Sometimes |
| Reflexes | ||
| Deep tendon reflexes | Hyperactive‡ | Hypoactive |
| Plantar | Babinski sign(s) | Absent |
| Sensory loss | Patterns* | Hands and feet |
*Examples: motor and sensory loss of one side or lower half of the body (e.g., hemiparesis or paraparesis), and hemisensory loss.
MS appears to be a partial exception to the rule that CNS demyelinating damage is permanent. In MS, episodes of demyelination of several CNS areas, including the optic nerves, partially or even completely resolve (see Chapter 15). However, the improvement results from resolution of myelin inflammation rather than myelin regeneration. When MS-induced demyelination eventually encompasses large areas of cerebral CNS myelin, it results in permanent quadriparesis and dementia.
Diabetes
Patients with diabetic neuropathy may also have autonomic nervous system involvement that causes gastrointestinal immobility, bladder muscle contraction, and sexual dysfunction. In fact, erectile dysfunction is occasionally the first or most disturbing symptom of diabetic autonomic neuropathy (see Chapter 16).
Toxic-Metabolic Disorders
Chronic, low-level intoxication by several other heavy metals causes polyneuropathy, dermatologic abnormality, and mental changes. In contrast, acute heavy metal poisoning typically leads to fatal gastrointestinal symptoms and cardiovascular collapse. Arsenic, which is tasteless and odorless, is a poison used in popular murder cases. With chronic, low-level, deliberate, accidental, or industrial intoxication, arsenic causes anorexia, malaise, and a distal neuropathy that might mimic Guillain–Barré syndrome. It also causes several characteristic dermatologic abnormalities: Mees lines on the fingernails (Fig. 5-6), hyperpigmentation, and hyperkeratosis.
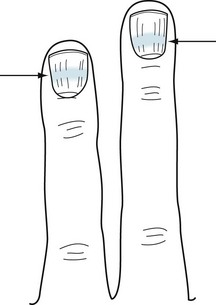
FIGURE 5-6 Mees lines, white bands (arrows) that stretch across the fingernails, characteristically indicate arsenic poisoning. In addition, poisoning by other heavy metals and trauma can cause them.
Mercury intoxication is more complex than arsenic poisoning. Individuals with mercury poisoning may develop a neuropathy and various CNS deficits, including cognitive impairment, ataxia, dysarthria, and visual field changes. Their gums accumulate a telltale dark line just below their teeth (Fig. 5-7).
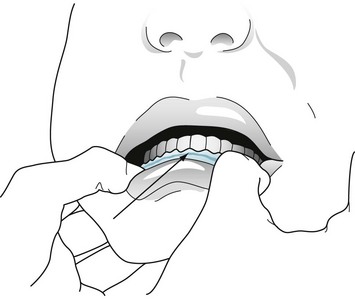
FIGURE 5-7 Chronic mercury poisoning causes a dark blue or black line (arrow) along the gum. Individuals with this sign usually also have neuropathy and central nervous system signs, such as ataxia and dysarthria.
Investigators at one time proposed that mercury-based dental amalgams (“fillings”) caused Alzheimer disease and other neurodegenerative illnesses either by dissolving in saliva and allowing mercury to enter the circulation or emitting a mercury vapor those individuals inhaled. In another inquiry, because ethyl mercury was a major component of the common vaccine preservative, thimerosal, investigators suspected that routine childhood immunizations caused autism (see Chapter 13). However, statistically powerful epidemiologic studies disproved both of those suspicions. In the case of vaccinations, the original “investigators” possibly engaged in fraud.
Neuropathies With Comorbid Mental Status Changes
Although most neuropathies, as described in the previous section, may be painful, incapacitating, or even devastating to the PNS, they generally do not cause mental changes in adults. For example, most people who are old, diabetic, on hemodialysis, or receiving chemotherapy remain intelligent, thoughtful, and competent even though beset by pain, sensory loss, and weakness. In contrast, only a few diseases (see Box 5-1) cause the combination of dementia and neuropathy, which would indicate both cerebral cortex and peripheral nerve damage. An analogous combination would be dementia and movement disorders, which would indicate cerebral cortex and basal ganglia damage (see Box 18-4).
Nutritional Deficiencies
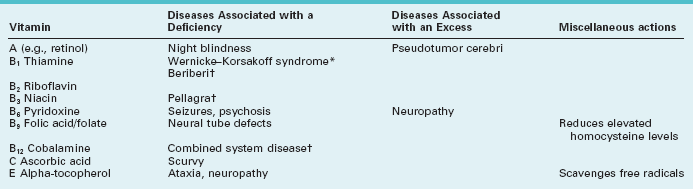
Deficiencies of thiamine (vitamin B1), niacin (nicotinic acid, B3), or vitamin B12 (cobalamine), each produce a predominantly sensory neuropathy accompanied by dementia or other mental status abnormality (Table 5-3). From a worldwide perspective, starvation has been the most common cause of deficiencies of vitamins, their carrier fats, minerals, and other nutrients. For example, beriberi was the starvation-induced neuropathy attributable to thiamine deficiency endemic in eastern Asia. In the United States, alcoholism, bariatric surgery, and malabsorption syndromes have replaced starvation as the most common causes of nutritional neuropathies. Curiously, few patients with anorexia nervosa or self-imposed extreme diets develop a neuropathy. Their protection may lie in a selective, possibly secret, intake of food or vitamins.
Bariatric surgery remains a unique example. After its rapid introduction and widespread acceptance, postoperative “micronutrient” deficiencies caused various neurologic illnesses. Thiamine, copper, and vitamins B12 and E deficiencies frequently caused neuropathy, but also occasionally encephalopathy or myelopathy (see Chapter 4), i.e., CNS problems. Routine postoperative administration of these micronutrients has prevented the problem.
Whatever the cause, thiamine deficiency generally leads to absent DTRs and loss of position sensation. In fact, until patients walk in the dark, when they must rely on position sense generated in the legs and feet, their deficits may remain asymptomatic. In the well-known Wernicke–Korsakoff syndrome, amnesia, dementia, and cerebellar degeneration accompany the neuropathy associated with alcoholism (see Chapter 7).
Among its many functions, vitamin B12 sustains both CNS and PNS myelin. Thus, B12 deficiency leads to the combination of CNS and PNS damage – combined system disease. Although its manifestations include a neuropathy, cognitive impairment and sensory loss reflecting demyelination of the posterior columns of the spinal cord (see Fig. 2-19B) predominate. Patients also develop a characteristic megaloblastic anemia. Most importantly, neurologists refer to combined system disease as a “correctable cause of dementia” because B12 injections can reverse the cognitive impairment as well as the other CNS and PNS manifestations. The usual causes of B12 deficiency include pernicious anemia, malabsorption, a pure vegetarian diet, or prolonged exposure to nitrous oxide, a gaseous dental anesthetic. (Nitrous oxide inactivates B12 by oxidizing its cobalt.)
The screening test for B12 deficiency consists of determining the serum B12 level. In equivocal cases, especially when cognitive impairment or spinal cord abnormalities are not accompanied by anemia, determining the serum homocysteine and methylmalonic acid levels can corroborate the diagnosis: in B12 deficiency, both homocysteine and methylmalonic acid levels rise to abnormally high levels (Fig. 5-8). Intrinsic factor antibodies, a classic finding in pernicious anemia, will be detectable in only about 60% of cases. The standard confirmatory test is the Schilling test.
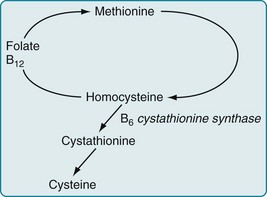
FIGURE 5-8 Vitamin B12, acting as a coenzyme, along with folate, facilitates the conversion of homocysteine to methionine. Other enzymes complete the cycle by converting methionine back to homocysteine. An absence of B12 leads to the accumulation of both methionine and homocysteine. Whatever the cause, an elevated homocysteine level is a risk factor for neural tube defects, cerebrovascular and cardiovascular disease, and other neurologic conditions.
In contrast to malnutrition causing neuropathy, excessive intake of certain vitamins causes neurologic problems. For example, although the normal adult daily requirement of vitamin B6 (pyridoxine) is only 2–4 mg daily, several food faddists who consumed several grams daily as part of a special diet developed a profound sensory neuropathy. Similarly, high vitamin A intake may cause pseudotumor cerebri (see Chapter 9) or induce fetal abnormalities (see Chapter 13).
Infectious Diseases
Several common organisms have a predilection for infecting the peripheral nerves and sparing the CNS. For example, herpes zoster infects a single nerve root or a branch of the trigeminal nerve, usually in people older than 65 years or those with an impaired immune system. An infection with herpes (Greek, herpes, spreading skin eruption) causes an ugly, red, painful, vesicular eruption (“shingles”) that may remain excruciating long after the skin infection has resolved (see postherpetic neuralgia, Chapter 14). As another example, leprosy (Hansen disease), infection with Mycobacterium leprae, causes anesthetic, hypopigmented patches of skin, anesthetic fingers and toes, and palpable nerves. It particularly affects the cool portions of the body, such as the nose, earlobes, and digits; however, depending on its variety, the infection strikes the ulnar or another large nerve either singly or along with others.
Acute Lyme disease typically produces multiple problems, such as arthritis, malaise, low-grade fever, cardiac arrhythmias, and a pathognomonic bull’s-eye-shaped expanding rash, erythema migrans (Greek, erythema, flush + migrans, move), surrounding the tick bite. In addition, Lyme disease frequently causes a facial nerve paresis, similar to Bell’s palsy, either unilaterally or bilaterally (see Fig. 4-15). Its PNS manifestations range from a mild neuropathy causing only paresthesias to a severe Guillain–Barré-like illness.
With CNS involvement, patients typically have headache, delirium (see Chapter 7), and other signs of meningitis or encephalitis. Their CSF may show a pleocytosis, elevated protein, decreased glucose concentrations, and Lyme antibodies. Serologic tests for Lyme disease remain unreliable. Another confusing aspect of the diagnosis is that patients may have a biologic false-positive test for syphilis because B. burgdorferi is a spirochete (see Chapter 7).
Numerous individuals and physicians attribute years of symptoms – cognitive impairment, weakness, fatigue, and arthralgias – after an attack of adequately treated Lyme disease to a persistent Lyme infection or disordered immunologic response to it. This condition, “chronic Lyme disease,” meets with skepticism in the neurologic community because it lacks consistent clinical criteria, pathology, and test results. Moreover, chronic Lyme disease symptoms do not respond to additional antibiotic treatment (see Chapters 6 and 7).
Inherited Metabolic Illnesses
Although numerous genetically determined illnesses cause neuropathy, two also cause psychosis.
Metachromatic leukodystrophy (MLD), an autosomal recessive illness carried on chromosome 22, derives its name from the colored granules (lipid sulfatides) that accumulate in the lysosomes of the brain, peripheral nerves, and many nonneurologic organs, such as the gallbladder, pancreas, and liver. Most importantly, MLD, like MS, causes a demyelination process in the CNS white matter (leukodystrophy) and, to a lesser extent, the PNS (see Chapter 15).
MLD symptoms usually first appear in infants and children, in whom the illness pursues a rapidly fatal course. In young adults, MLD presents with personality and behavioral changes, thought or mood disorder, and cognitive impairment. MLD-induced cognitive impairments typically progress slowly to dementia. Neurologists describe MLD-induced cognitive impairment as a “frontal dementia” because of its combination of personality, behavioral, and cognitive manifestations (see Chapter 7). Peripheral neuropathy and signs of CNS demyelination – spasticity and ataxia – follow and eventually overshadow the frontal dementia.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


