Chapter 18 Peripheral Nerve Stimulation
Percutaneous Technique
 Minimally invasive PNS is a novel technique that may allow a trial of peripheral nerve stimulation before permanent placement and potentially allow long-term implantation.
Minimally invasive PNS is a novel technique that may allow a trial of peripheral nerve stimulation before permanent placement and potentially allow long-term implantation.






 Preimplantation nerve block is extremely useful in patient selection, particularly if the patient receives complete relief of pain in a single nerve distribution.
Preimplantation nerve block is extremely useful in patient selection, particularly if the patient receives complete relief of pain in a single nerve distribution.


 Transmuscular placement is undesirable and with muscular movement may cause a ratcheting effect and promote migration.
Transmuscular placement is undesirable and with muscular movement may cause a ratcheting effect and promote migration.


Introduction
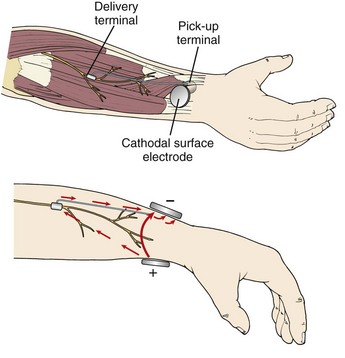
Peripheral nerve stimulation (PNS) is a technique of direct electrical stimulation of peripheral nerve(s) to relieve pain or to assist with the functional restoration of patients with severe neurological injuries, including those to the spinal cord. The term PNS has also been used to describe the superficial placement of electrical leads in areas of the body such as the back, thorax, or abdomen where no discrete named nerves exist but small nerve fibers near the dermis can be targeted to produce local analgesia. This type of stimulation is mechanistically poorly understood and will be referred to as peripheral field stimulation (not the subject of this chapter). PNS became conceptually possible after the development of the gate control theory.1 Wall and Sweet’s experiments with PNS tested the concept of electrical stimulation–produced analgesia, initially of the authors’ infraorbital nerves and subsequently in eight patients.2 Soon many neurological and orthopedic surgeons became interested in the technique, and several case series of these peripheral nerve surgeries were described 3–6 The early history of the development of these techniques is chronicled by Michael Stanton-Hicks and colleagues,6 who describe the indications, outcomes, and complications of a series of 91 patients at the Cleveland Clinic. Despite early investigator interest and the development of novel lead and battery technology, innovations in programmability, and other technical improvements for stimulation of the peripheral nerves, the application and study of PNS has been less vigorous in scope than that for spinal cord stimulation. The absence of a comparable minimally invasive trial system that became available with the introduction of percutaneous spinal cord stimulation electrodes in the 1980s may be one reason that peripheral nerve surgeries have not advanced as rapidly. Other potential reasons for decreased interest in PNS may be frequent complications such as lead migration (requiring revision surgery), neurological damage to the axons from mechanical or stimulation-induced nerve injury, and poor patient selection leading to poor outcomes. PNS has always been an open technique since its inception more than 40 years ago, but recently minimally invasive techniques were described.7–9 Possible advantages to peripheral nerve stimulator placement via a minimally invasive technique might include: (1) minimal nerve trunk dissection and manipulation (potential trauma); (2) the omission of the need for a fascial graft or fat pad interposed between the electrode and the nerve (the fat around the epineurium in situ is minimally perturbed by the percutaneous electrode); (3) a true percutaneous trial avoiding dissection and open surgery; and (4) the ability to perform intraoperative electrical stimulation testing in an awake patient with minimal sedation compared to a patient under general anesthesia. Cadaver feasibility studies were performed in 2008,7,8 suggesting that ultrasound (US) image guidance might allow safe placement of peripheral nerve stimulating electrodes near target peripheral nerves, similar to nerve catheter placement. Following these feasibility studies, a case series of nine patients who received PNS placements using US was published, based on the principles described in the cadaver studies.9 In two of the nine cases, patients with good paresthesia coverage did not achieve analgesia and were not implanted, thus avoiding an unnecessary surgical dissection. Most cases produced durable analgesia beyond 1 year. The programming of multiple different stimulation parameters intraoperatively allowed the additional placement of second electrodes parallel to the first or on either side of a nerve trunk to more optimally stimulate the desired fascicles in some cases (Fig. 18-1).9 Others have described a stimulus router concept that eliminates the need for an implanted generator. A surgeon places a passive implant delivery terminal near the target nerve. Current is passed between a surface cathodal electrode and a pick-up terminal, a small fraction of which (10% to15%) is passed to the delivery terminal. This results in PNS at threshold. It is unclear at this time if this type of implant would be less prone to migration without additional study (Fig. 18-2).10