♦ Preoperative
Imaging
- Cervical spine magnetic resonance imaging (MRI)
- Cervical spine computed tomography (CT) (to evaluate for ossification of the posterior longitudinal ligament)
- Cervical spine flexion-extension plain films
Equipment
- Choose laminoplasty system: ceramic spacers, titanium miniplates, etc.
- Operating loupes or microscope
Spinal Monitoring
- Somatosensory evoked potentials and electromyography monitoring are commonly used in cervical myelopathy cases
- General endotracheal anesthesia, consider fiberoptic intubation
- Review specific anesthetic management (e.g., no paralytics for monitoring nerve roots).
- Spinal monitoring leads should be placed prior to positioning. In cases of myelopathy or severe canal stenosis, baseline somatosensory evoked potentials are often obtained prior to positioning.
- Foley catheter is generally inserted.
- Intravenous antibiotics are administered.
♦ Intraoperative (Fig. 104.1)
Positioning
- Position patient prone with all appropriate pressure points supported
- Protect the axilla to prevent brachial plexus stretch injury
- Lateral intraoperative fluoroscopy is used to identify the operative levels and to confirm neutral or lordotic alignment of the cervical spine
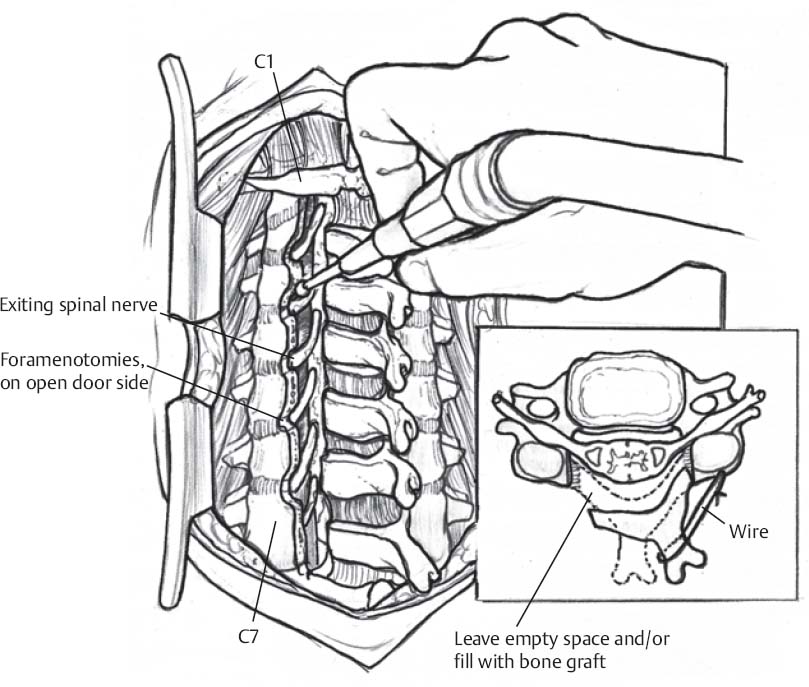
Fig 104.1 Schematic of cervical laminoplasty performed with high-speed drill.
Only gold members can continue reading. Log In or Register to continue
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


