♦ Preoperative
Operative Planning
- Magnetic resonance imaging (MRI) scan
- Computed tomography (CT) myelogram if MRI not possible, equivocal or for reoperation
- Preoperative planning: selection of implant type and possibly size
- Height of disc space
- Bone quality
- Height of disc space
- Flexion/extension films
- Preoperative CT scan for navigation
- Decision on open versus minimal access technique; depends on surgeon experience, preference, and patient anatomy
- Decision on fusion strategy: autograft or allograft bone, fusion enhancing substances, bone morphogenic protein (BMP), bone marrow
- Jackson table (radiolucent table)
- C-arm fluoroscopy
- Isocentric (Iso-C) for three-dimensional (3D) imaging; can be used as regular fluoroscopy, to check screw placement intraoperatively, or for stereotactic navigation
- Instrumentation for open or minimal access surgery, implants, fusion material: autograft or allograft bone, BMP, etc.
- Microscope (surgeon preference) and/or loupes and headlight
- High-speed drill
- Cobb retractors
- Tools for discectomy, preparation of endplates, and insertion of interbody implant (surgeon preference)
- Intraoperative monitoring of electromyography/somatosensory evoked potentials
- Operating room set-up
- Jackson table with chest and hip support
- Regular fluoroscopy or Iso-C, screen across from surgeon
- Microscope (surgeon preference)
- Stereotactic navigation system (surgeon preference)
- Cell saver (multilevel surgery)
Anesthetic Issues
- Intravenous antibiotics 30 minute preoperative
- Monitoring: arterial line, large bore venous access
- Foley catheter
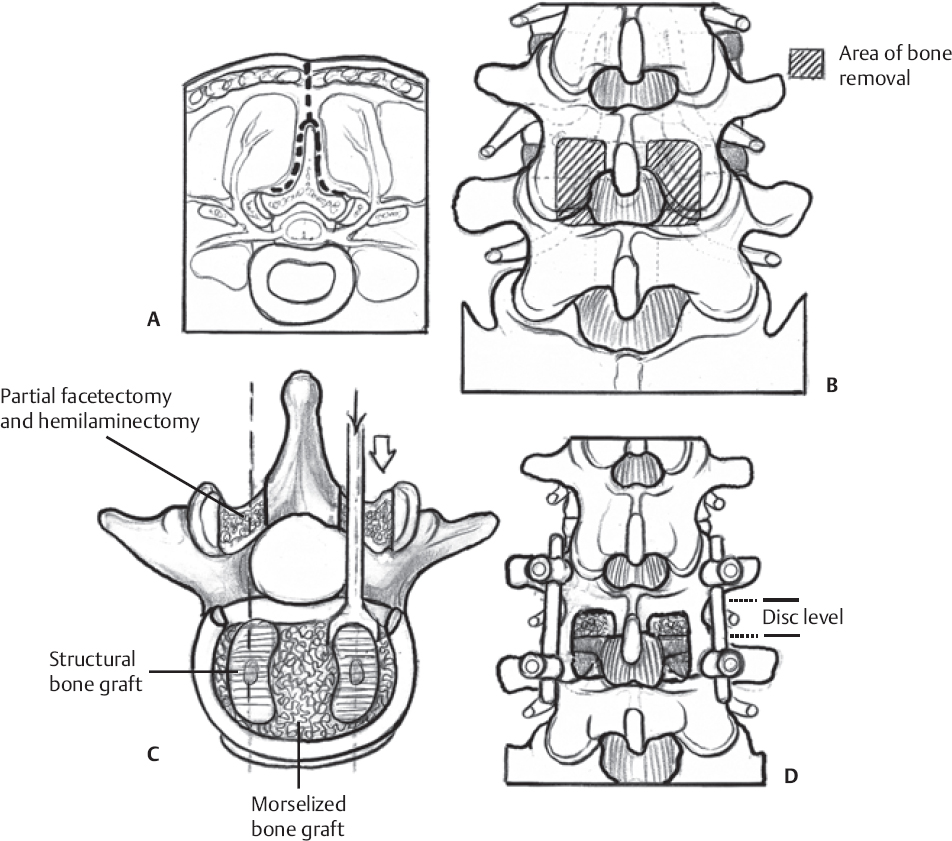
♦ Intraoperative (Fig. 123.1)
Positioning
- Prone on Jackson table
- Lumbar spine in lordosis
- Avoid neck hyperextension
- Padding of arms and legs
- Venous compression devices
Mark Incision
- Identify correct level with fluoroscopy
- Midline skin incision ~10cm
- Mark iliac crest on skin for possible bone graft/bone marrow harvesting
- Scrub and prep
- As per institution/surgeon preference
Exposure
- Bilateral subperiosteal muscle dissection to expose both laminae and trans verse processes. Use Cobb retractors and pack wound frequently with lap sponges to minimize bleeding and blood loss. Clearly identify transverse processes above and below disc space and place deep retractors.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


