♦ Preoperative
Imaging
- P lain x-rays
- Determine number of ribs for localization
- Assess deformity and/or instability
- Determine number of ribs for localization
- Magnetic resonance imaging (MRI)
- Determine extent of neural element compression
- Computed tomography
- Evaluate bony anatomy
- Computed tomography/myelogram
- If MRI contraindicated
Operative Planning
- Patient counseling regarding risk, benefits, and postoperative course
Routine Equipment
- Basic spine tray including Kerrison rongeurs (2 to 4 mm)
- Cautery—monopolar and bipolar
- High-speed drill (e.g., Midas Rex)
- Headlight and loupe magnification
Special Equipment
- Cell Saver (Haemonetics, Braintree, MA)—if significant blood loss is anticipated in the absence of infection/neoplastic disease
- Microscope for intradural pathology
Operating Room Set-up
- Prone table: Jackson table with Wilson frame or bolsters
- Mayfield head holder versus Gardner-Wells tongs with traction
- Intraoperative anteroposterior and lateral x-ray versus fluoroscopy
Anesthetic Issues
- Secure endotracheal tube for prone position
- Appropriate blood pressure monitoring
- Foley catheter for extended cases (beyond 3 hours)
- Perioperative antibiotics 30 minutes prior to skin incision
- Perioperative steroids for decompressive or intradural pathology
- Avoid any orbital compression if patient’s face is placed on cushioned mask
♦ Intraoperative (Fig. 108.1)
Positioning
- Prone position
- Arms tucked along side for pathology rostral to T6–T7
- Head secured with Mayfield head holder or Gardner-Wells tongs and 15 pounds of traction
- Arms abducted and placed on cushioned boards for pathology caudal to T6–T7
- Arms tucked along side for pathology rostral to T6–T7
- Maintain exposure of posterior iliac crest if fusion intended.
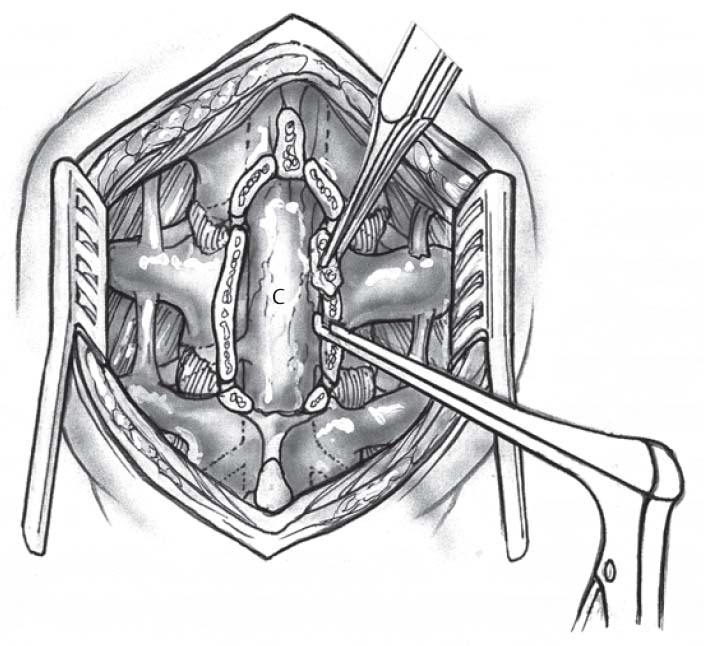
Fig 108.1 Schematic of posterior thoracic approach and decompression. Dorsal decompression with removal of spinous processes and laminae. C, spinal cord.
Only gold members can continue reading. Log In or Register to continue
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


