Prepontine Cistern Mass
Gregory L. Katzman, MD, MBA
DIFFERENTIAL DIAGNOSIS
Common
CSF Flow Artifact
Dolichoectasia (Vertebrobasilar)
Fusiform Aneurysm, ASVD
Meningioma
Metastases, Skull and Meningeal
Less Common
Epidermoid Cyst
Chiari 2 (“Creeping Cerebellum”)
Exophytic Brainstem Glioma, Pediatric
Pituitary Macroadenoma (Giant)
Neurocysticercosis
Intracranial Hypotension
Rare but Important
Inflammatory Mass
Tuberculosis
Fungal Diseases
Neurosarcoid
Clival Neoplasms
Chordoma, Clivus
Chondrosarcoma, Skull Base
Plasmacytoma, Skull Base
Nasopharyngeal Tumor (Invading Clivus)
Schwannoma
Arachnoid Cyst
Craniopharyngioma
Neurenteric Cyst
Ecchordosis Physaliphora
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Anatomy
Extensive CSF space along ventral & lateral pons, dorsal to clivus (a.k.a, pontine cistern)
Bounded superiorly by interpeduncular cistern, inferiorly by subarachnoid space of spinal cord, & continuous about medulla with cerebellomedullary cistern
Many abnormalities, often from transpatial processes
Helpful Clues for Common Diagnoses
CSF Flow Artifact
MR artifacts divided into 2 categories: Time-of-flight effects & turbulent flow
Worsens with thinner slices, longer TE, and imaging perpendicular to flow
Assess real vs. artifact in other planes
Minimize TOF losses: Use short TE, image parallel to flow, acquire thicker slices
Dolichoectasia (Vertebrobasilar)
Older patients
Look for ASVD in other vessels
Ectasia often extends into branches
May have significant mass effect on pons
Fusiform Aneurysm, ASVD
Long segment fusiform arterial dilatation
Involves long nonbranching segments
Calcifications common
Lumen enhances strongly, clot does not
Meningioma
Clival dural-based enhancing mass
Infratentorial (8-10%): CPA most common
Causes cranial neuropathies or ataxia
Metastases, Skull and Meningeal
Enhancing lesion(s) with skull/meningeal destruction/infiltration
Manifestations: Smooth thickening, nodularity, loculation, fungating masses
Image entire neuraxis!
Helpful Clues for Less Common Diagnoses
Epidermoid Cyst
Usually extends medially from CPA cistern
Lobulated, irregular, insinuating CSF-like mass
Doesn’t completely suppress on FLAIR; restricts on DWI
Chiari 2 (“Creeping Cerebellum”)
Small posterior fossa with low torcular herophili
Cerebellar hemispheres/tonsils herniate anteriorly → “creeping”
Pons, cranial nerve roots often elongated
Exophytic Brainstem Glioma, Pediatric
Nonenhancing mass markedly expanding pons; may engulf basilar artery
Infiltrative have poor survival
Focal are uncommon, better prognosis
Pituitary Macroadenoma (Giant)
No distinct pituitary gland
Bone CT shows benign bony margins
Early intense but heterogeneous CTST+
Dural “tail” may mimic meningioma
Neurocysticercosis
Cisterns > parenchyma > ventricles
Basal cistern cysts may be racemose
Cysts variable, typically 1 cm, range from 5-20 mm, contain a 1-4 mm scolex
Most are isointense to CSF
Intracranial Hypotension
Sagittal shows brain descent in 40-50%
Pons may be compressed against clivus
Diffusely, intensely enhancing dura in 85%
Bilateral subdural fluid collections in 15%
Helpful Clues for Rare Diagnoses
Inflammatory Mass
Tuberculosis
Basilar meningitis, pulmonary TB
Thick basilar exudate ± tuberculomas/abscesses
Fungal Diseases
Blastomycosis, coccidiomycosis, histoplasmosis, candidiasis
Meningeal enhancement, multiple enhancing brain lesions
Neurosarcoid
Classically infiltrates dura, leptomeninges, basal cisterns
Solitary or multifocal CNS mass(es) ± abnormal CXR
Clival Neoplasms
Chordoma, Clivus
Destructive midline mass centered in clivus with high T2 signal intensity
Sagittal images show tumor “thumb” indenting anterior pons
Chondrosarcoma, Skull Base
Arises from petro-occipital fissure
May extend posteriorly into prepontine cistern
Hyperintense on T2WI, enhances strongly but heterogeneously
Chondroid mineralization on CT (50%)
Plasmacytoma, Skull Base
Solitary intraosseous osteolytic soft tissue mass with non-sclerotic margins
Peripherally displaced osseous expansion/fragmentation may be seen
Nasopharyngeal Tumor (Invading Clivus)
Often squamous cell CA arising from nasopharyngeal mucosal space
Multi-planar MR images best show invasion of clivus
Schwannoma
T2 hyperintense, enhance
Arachnoid Cyst
Extra-axial cyst follows CSF attenuation/signal
Suppresses completely with FLAIR; no DWI restriction
Craniopharyngioma
90% Ca++, 90% cystic, 90% enhance
May extend behind sella into posterior fossa
Neurenteric Cyst
Round/lobulated nonenhancing, slightly hyperintense to CSF mass
Benign malformative endodermal CNS cyst
Ecchordosis Physaliphora
Notochord remnant
Extends from clivus into prepontine cistern
Hyperintense on T2WI
Image Gallery
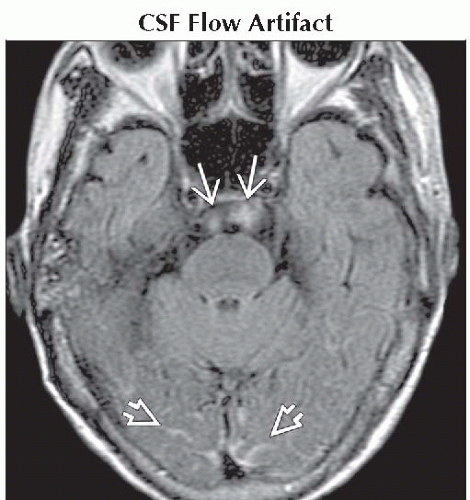 Axial FLAIR MR reveals a hyperintense artifact  due to CSF turbulent flow. Also note sulcal hyperintensity from subarachnoid hemorrhage due to CSF turbulent flow. Also note sulcal hyperintensity from subarachnoid hemorrhage  . . |
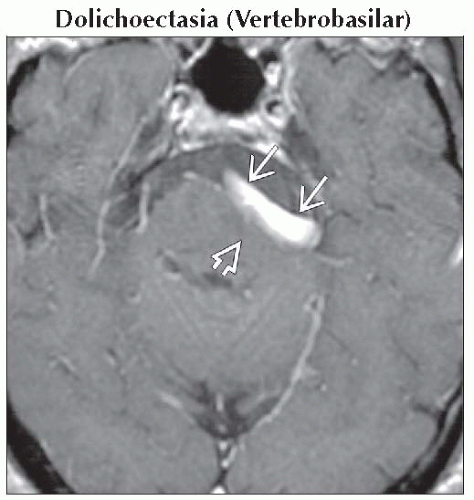 Axial T1 C+ MR demonstrates luminal enhancement of a dolichoectatic basilar artery  with associated deformation of the pons with associated deformation of the pons  . . |
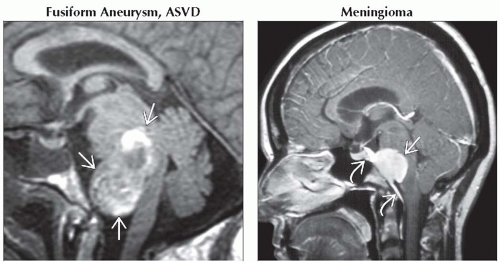 (Left) Sagittal T1WI MR shows a large mass anterior to the pons and medulla
 . Note mixed hyper-, isointense signal caused by slow flow & laminated clot in this classic ASVD fusiform aneurysm. (Right) Sagittal T1 C+ MR demonstrates avid meningioma enhancement . Note mixed hyper-, isointense signal caused by slow flow & laminated clot in this classic ASVD fusiform aneurysm. (Right) Sagittal T1 C+ MR demonstrates avid meningioma enhancement  as well as enhancing dural tails as well as enhancing dural tails  . .Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|