In recent years, major epidemiological surveys have been carried out in the community in many different countries, in the United Kingdom most recently by the Office of National Statistics (to find this and other surveys go to http://www.statistics.gov.uk/ STATBASE/Product.asp?vlnk=8258). The findings in such community surveys can be compared with findings in primary care surveys, when it will be found that the list of common mental disorders is not quite the same, although conditions characterized by symptoms of depression and anxiety are the most common. Rather than considering the detailed diagnoses, it can be helpful to distinguish between ‘internalizing disorders’, which besides anxiety states and depression, also include the fear disorders like phobias and panic disorder, obsessive-compulsive disorder and many cases of somatization disorder; and ‘externalizing disorders’ consisting of conduct disorder in childhood, and antisocial behaviour, as well as drug and alcohol disorders in adult life. The former group of disorders are characterized by subjective distress, and typically high levels of anxious and depressive symptoms; while in the latter group abnormalities are in externally observed behaviour.(1)
In community surveys it can be seen that rates of internalizing disorders rise sharply after puberty, are highest between the ages of 35 and 55 and fall thereafter, and that females rates are higher than males at all ages., while rates of externalizing disorders reach their maximum between the ages of 15 and 34, and fall sharply after that, with males rates much higher than female rates at all ages. This is shown in Table 7.8.1 (which does not include antisocial behaviour as reliable data are not available in the community).
The Goldberg-Huxley Model(2)
This was devised as a framework for comparing the characteristics of patients seen in the community with those in other medical settings, and describing the pathway which people usually follow to mental health care in places where GPs act as ‘gatekeepers’. It consists of five levels, separated by four filters. The figures for psychiatric morbidity over 1 year necessitate using estimates of incidence rates, and are therefore much higher than the point prevalence rates reported in community surveys. The essence of the model is the demonstration that most distressed patients will see a doctor over the course of 1 year (filter 1), but only about half of them will have their distress detected (filter 2). Most common mental disorders are treated in primary care, so filter 3 is relatively impermeable, only allowing one in five to pass. Psychiatrists only have any part in the process with the fourth filter, which also holds back most patients. Psychiatrists therefore form their ideas about mental disorders from a highly skewed section of all those with disorders.
Prevalence of psychiatric disorder in primary care
In the United Kingdom, about 80 per cent of the population consult their doctor in the course of a year, and prevalences among attenders are higher than among the general population.(2) In contrast, specialist mental health services see between 1 and 2 per cent of the population in the course of a year, and admit only about 0.5 per cent to inpatient care, so that primary care deals with the major part of the burden of common mental disorders.
The World Health Organization (WHO) carried out the largest primary care survey in 14 countries(3) but for purposes of comparison only the UK data will be shown here. Table 7.8.2 compares the frequencies and types of mental disorders seen in the community, in primary care, and in psychiatric practice. Mental disorders seen in primary care settings are more severe on average than those seen in community surveys, and different disorders predominate. The figures shown are for practices in Manchester with a fairly high prevalence of mental disorders, but the spread of diagnoses is fairly similar in other countries. The ICD-10 criteria only counted somatoform disorders if they were severe and long-standing, and do not count the many patients presenting with unexplained somatic symptoms, which are often accompanied by symptoms typical of anxiety or depression. A more recent study from Denmark(4) has estimated that almost a half of their patients were diagnosed cases of mental disorders, with somatoform disorders being found in about one-third. Patients with established physical illnesses are also at greater risk of mental disorders, and this is especially so if they are disabled by their illness. It can be seen from Table 7.8.3 that disorders admitted to psychiatric hospitals in the United Kingdom are different again from those typically seen in primary care, with organic states, drug and alcohol dependence, schizophrenia and severe depressive states accounting for the majority of cases (Source: http://www.hesonline.nhs.uk/Ease/ servlet/ContentServer?siteID=1937&categoryID=202).
Table 7.8.1 Annual prevalence of mental disorders in the community by type and age, rates per 100 at risk
Disorder
Gender
5 to 16
to 34
to 54
to 74
All (16-75)
Internalizing
Male
3.1
11.70
16.75
9.87
13.5
Female
4.3
20.55
21.35
14.80
19.4
Externalizing
Male
10.05
11.6; 18.9
2.25; 10.4
0.4; 3.8
6.0; 11.9
Female
4.35
5.3; 5.7
0.75; 2.1
0.4; 0.5
2.3; 2.9
Other
Male
1.9
0.33
0.78
0.23
0.5
Female
0.75
0.42
0.73
0.52
0.6
Internalizing = any neurotic disorder. Externalizing = conduct disorder for age 5-16; for the remaining age groups the rate for drug dependence is shown first, followed, after the semicolon, by the rate for alcohol dependence. Other = psychotic disorders in adults. Source: National Statistics website: www.statistics.gov.uk Crown copyright material is reproduced with the permission of the Controller Office of Public Sector Information (OPSI).
Table 7.8.2 Prevalence of mental disorder by gender for the community, for primary care attenders, and for admissions to psychiatric beds
The community annual prevalence (%)
Primary care cases consecutive attenders (%)
Mental hospital inpatients (%)
Males
Females
Males
Females
Males
Females
Mixed anxiety depression
6.8
10.8
2.1
4.5
9.8
17.6
GAD
4.3
4.6
4.9
14.9
Panic
0.7
0.7
3.4
3.6
Phobias
1.3
2.2
2.1
4.6
Neurasthenia
–
–
6.1
21.7
Somatoform disorder
–
–
–
0.5
OCD
0.9
1.3
–
–
Depression
2.3
2.3
13.9
18.3
17.9
27.3
Alcohol dependence
11.9
2.9
5.3
0.8
Drugs dependence
5.4
2.1
–
–
30.1
14.3
Schizophrenia
0.6
0.5
–
–
20.4
13.7
Organic, dementia
–
–
–
–
10.3
15.9
Subnormality
–
–
–
–
7.1
5.4
Developmental disorders
–
–
–
–
5.1
5.4
Any Dx
14.1%
19.9%
23.5%
27.5%
100%
100%
Sources: National Statistics website: www.statistics.gov.uk Crown copyright material is reproduced with the permission of the Controller Office of Public Sector Information (OPSI).
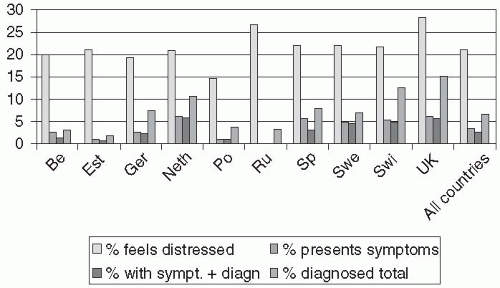
A study in 10 European countries shows 28 per cent of consecutive attenders in the United Kingdom to be distressed on a screening interview, but only 6 per cent presented psychological symptoms to their GP. Most of these (5.5 per cent) received a psychiatric diagnosis, but the GPs also diagnosed others as ‘psychiatric’—so that their total rate was 15 per cent.(5) These figures are fairly similar to those in Switzerland and the Netherlands, but in stark contrast to those in Eastern Europe. In the Russian Federation, for example, 27 per cent were distressed, but none reported psychological distress to their GPs, and none were diagnosed: however, the GPs identified 3 per cent of their patients as ‘psychiatric’. Fairly similar figures were reported in Estonia, Poland, and Belgium; while figures in Germany, Spain, and Sweden are intermediate (ibid 2007; see Fig. 7.8.1). This study also showed that GPs who discuss psychosocial matters with their patients, and look at them are better at diagnosing them—a finding that echoes previous research in the United Kingdom.(2)
It can be seen from Fig. 7.8.1 that most distressed patients—who may well be found to have a mental disorder if interviewed with a research interview—do not mention their distress to their doctor, and that this accounts for failure to diagnose the disorder. Many patients who have not endorsed feelings of distress are nonetheless assessed as mental unwell, either because they are presenting with unexplained somatic symptoms or because they are under treatment for a mental disorder that has responded to treatment.
Table 7.8.3 The Goldberg-Huxley Model: Data for Manchester, UK
Level 1: Community samples
250-315/1000/year
First Filter: The decision to consult
Level 2: All those seeing GPs found to have a mental disorder
210-230/1000/year
Second filter: GPs ability to detect
Level 3: Cases recognized by the GP As ‘mental disorders’
101/1000/year
Third filter: GPs decision to refer
Level 4: All those seeing mental health professionals
20.6/1000/year
Fourth filter: Psychiatrist’s decision to admit to hospital
Level 5: Those admitted as inpatients
3.4/1000/year
(Note that these estimates are annual period prevalences, and depend on estimates of annual incidence rates in addition to point prevalence rates. Source: Reproduced from D.P. Goldberg and P.J. Huxley, Common mental disorders—a bio-social model, copyright 1992, The Tavistock Institute, London.)
Fig. 7.8.1 Proportions of population that feel distressed, present symptoms of distress, are diagnosed if they do so, and total number of patients diagnosed, in 10 European countries (Reproduced from P. Verhaak, J. Bensing, and A. Brink-Nuinen, Primary mental health care in 10 European countries: patients’ demands and GPs’ responses. European Journal of Psychiatry, 21, (1), Zaragoza Jan-Mar 2007, copyright 2007, INO REPRODUCCIONES, S.A.).
Clinical presentations
Somatization
Somatization is broadly defined as the expression of psychological distress through physical symptoms. In primary care, most patients present physical symptoms at the onset of an episode of anxiety and depression. This is actually the usual way that new episodes of common mental disorders present in general medical settings, as only about 15 per cent of new episodes present purely in psychological terms.(2)
Primary care somatizers can be subdivided into ‘facultative somatizers’, who admit to their psychological symptoms and accept a mental disorder diagnosis if appropriately interviewed, and ‘pure somatizers’ who, despite such an enquiry, still deny the presence of psychiatric symptoms. People have many reasons for preferring to present somatic symptoms to their doctors—they are understandably worried that they may have a new physical disease, they give priority to pains over other symptoms because it is pain that hurts, and they often wish to avoid the stigma of being thought psychologically distressed.
Somatizers may be compared with ‘psychologisers’, who directly present their psychological problems to their doctors. The former are more likely to report adverse childhood events and periods of childhood illnesses, while the latter have more abnormal attachment behaviours.
Hidden versus conspicuous morbidity
The ability of GPs to detect psychological disorders among their patients forms the second filter that patients must pass through in order to receive a diagnostic label. This ability varies a good deal between places as well as between disorders. In the WHO study(3) the overall average detection rate was 48.9 per cent, but rates varied from 75 per cent for Verona to 15.9 per cent for Shanghai (62.9 per cent for Manchester). Recognition rates for individual diagnoses followed these overall rates, with somatization disorder being best recognized, followed by depression. However, these detection rates do not reveal whether the GP is identifying the same patients as the research assessment. In fact, the exact agreement between the two (measured by κ) is rather poor, at only +0.18 for all centres (+0.38 for Manchester).
The second filter is passed when the GP recognizes a mental health problem in the patient, although this will often be without a precise ICD-10 diagnosis. Those recognized by the GP make up the ‘conspicuous’ morbidity—in fact, just under half of that estimated to be present in the waiting room population by a two-stage case-finding procedure: so that the patients who are not identified can be thought of as the ‘hidden morbidity’. These undetected patients continue to consult, but an outsider’s inspection of notes and prescriptions, or even discussion with the relevant doctor, will not identify them as patients with psychiatric morbidity. In practice, the ‘conspicuous’ morbidity may be greater than 50 per cent, as the longitudinal nature of primary care means that patients may be diagnosed in subsequent visits, and this is missed in cross-sectional waiting room studies.(6,7) Kessler et al. followed up a cohort of primary care patients over 3 years and found only 14 per cent of patients with depression remained unrecognized at the end of this period.(8) Rost et al. followed up 98 depressed patients who had made at least one visit to their GP and found 32 per cent were undetected at 1 year.(9) Despite this, GPs are good at recognizing severe depression, and unrecognized depression tends to be mild.(10,11,12) The severity of depression in primary care, rather than being defined categorically, may therefore be better conceptualized as running along a continuum from mild to severe. Using a dimensional approach Thompson et al. calculated GPs only miss one ‘probable’ case of depression every 29 consultations.(13)
Doctors better able to detect disorder have the following characteristics:(2)
Make eye contact with the patient
Make empathic comments
Pick up verbal cues
Pick up non-verbal cues
Ask directive questions, with a psychological content
Do not read notes, or look at their computer, while the patient is speaking
Deal with over-talkativeness
Deal with today’s problem
Data from the WHO study indicate that these ‘undetected illnesses’ are on an average less severe than those detected by GPs and have a somewhat better outlook. However, the data does not support the view that failure to detect these less severe disorders has serious long-term consequences for the patient(14) although this does not mean that there are not individuals would be better served if their distress was acknowledged.
Only gold members can continue reading. Log In or Register to continue