♦ Preoperative
Operative Planning
- Review imaging studies including radionucleotide studies
Equipment
- Mayfield head holder or horseshoe headrest
- Basic craniotomy tray
- High-speed drill
- Bone flap fixation tray
- Lumbar spinal drain
Operating Room Set-up
- Headlight and loupes
- Bipolar and Bovie cautery
Anesthetic Issues
- Preoperative intravenous antibiotics 30 min prior to incision
- Lumbar drain is inserted preoperatively
- Management of intracranial pressure: hyperventilation to pCO2 of 25 to 30 mm Hg, mannitol 0.5 to 1 g/kg intravenously starting at time of skin incision, propofol (if indicated)
♦ Intraoperative
Positioning
- Patient supine with neck flexed
Planning of Incision and Shave
- Bicoronal or modified bicoronal incision for approaches to anterior skull base
- With electrical clippers, a strip shave is performed approximately 1 cm in width over the planned incision
Sterile Scrub, Prep, and Drape
- As for standard craniotomy (see General Craniotomy, Chapter 2)
Incision and Scalp Flap
- Incision is infiltrated with lidocaine with epinephrine
- Operative timeout with anesthesia and nursing is performed to confirm procedure
- Incision is performed down through galea, sparing periosteum
- Raney clips or bipolar cautery are used to control scalp bleeding
- Scalp flap can usually be dissected free from temporalis muscle and reflected anteriorly without having to incise the temporalis fascia or muscle
- Pericranial flap is carefully dissected, reflected anteriorly, and wrapped in a moist gauze
Craniotomy and Extradural approach
- Depending on suspected location of CSF leak, a frontal or bifrontal craniotomy is performed.
- The dura is carefully elevated from the skull base and examined for obvious defects.
- Any defects are repaired by first circumferentially mobilizing the surrounding dura and then closing the defect primarily with 4–0 Nurolon reinforced with fibrin glue.
- If a defect cannot be repaired primarily, muscle, fascia, or a free flap of pericranium may be used as graft material to close the defect.
- Certain CSF fistulas (i.e, Middle cranial fossa) can be repaired by a primarily extradural approach (Fig. 68.1), while others will require intradural exploration
Intradural Exploration and Repair
- The dura is opened and reflected anteriorly
- CSF is removed from the lumbar drain in increments of 5 mL until adequate brain relaxation is obtained
- The frontal poles are gently retracted posteriorly to expose the floor of anterior fossa
- Any dural defects are visualized and repaired either intra- or extradurally
- The dural repair is reinforced with muscle, fascia, or a free flap of pericranium along with fibrin glue
- The dural incision is closed while the operative field is irrigated thoroughly to ensure adequate repair of all dural defects
- The pericranial flap is then placed between the dural defects and the floor of the anterior cranial fossa
- The pericranial flap is sutured to the dura with 4–0 Nurolon and the suture line is reinforced with fibrin glue
Cranialization of Frontal Sinus
- In general, if the posterior table of the frontal sinus is violated, then the sinus must be cranialized.
< div class='tao-gold-member'>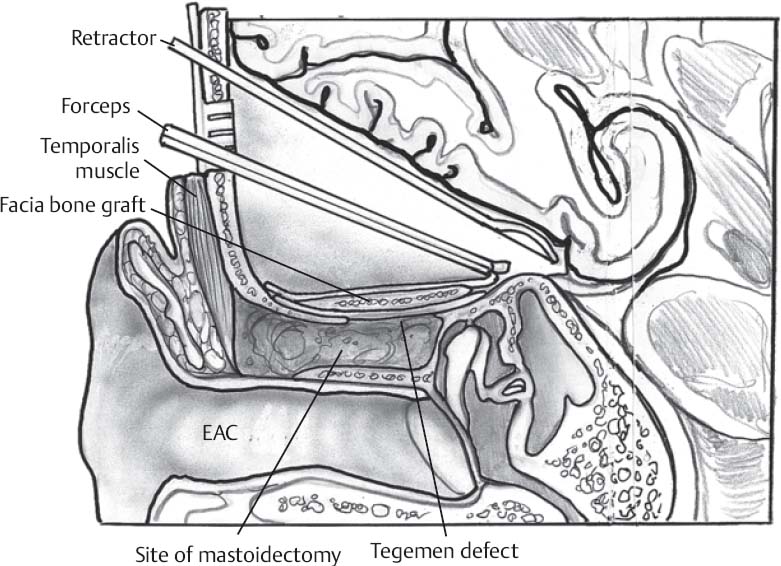 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


