♦ Preoperative
Imaging
- Magnetic resonance imaging to assess brain stem or spinal cord compression
- Plain x-rays to evaluate alignment
- Computed tomography with sagittal reconstructions to visualize extent of possible exposure (hard palate and vallecula)
Preoperative Care
- Somatosensory evoked potential/motor-evoked potentials may be useful
Equipment
- Self retaining anterior cervical retraction system
- Vessel loops may be useful to tag and reflect facial artery/vein and hypoglos-sal nerve.
Operating Room Set-up
- Nasal intubation may allow 1 cm additional jaw closure and increased exposure
- Somatosensory and motor-evoked potential monitoring (optional)
- Fluoroscopy (consider draping into field)
- Balanced microscope
Positioning
- Supine on operating table
- Head fixed in Mayfield head holder in slight extension and slight contralateral rotation
♦ Intraoperative
Exposure (Fig. 88.1)
- Horizontal incision 2 cm caudal to mandible line on right
- Divide platysma from midline to medial border of sternocleidomastoid
- Mobilize submandibular gland rostrally (see Fig. 88.1)
- Dissect out digastric and release from notch
- Identify facial artery and vein and protect laterally
- Identify hypoglossal nerve and protect
- Gently mobilize pharyngeal constrictor muscles to expose craniocervical junction
- Insert anterior cervical retractors (smooth blades)
- Confirm extent of exposure and midline with fluoroscopy
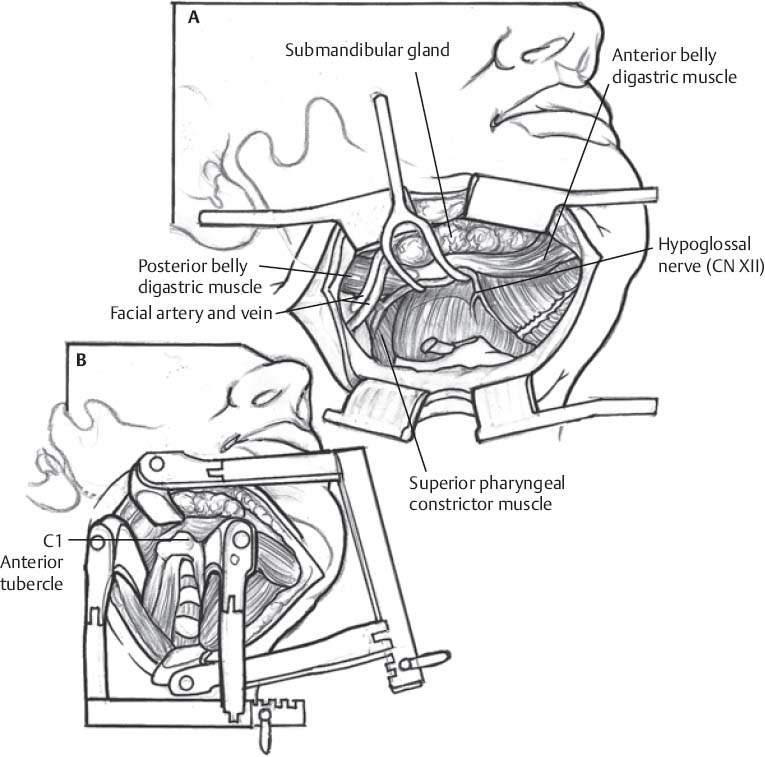
Fig. 88.1 Schematic of retropharyngeal approach, exposure, and critical structures. (A) Superficial exposure and (B) deep exposure.
Only gold members can continue reading. Log In or Register to continue
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


