Ring-Enhancing Lesion, Solitary
Yoshimi Anzai, MD, MPH
Judy Tan, MD
DIFFERENTIAL DIAGNOSIS
Common
Metastases, Parenchymal
Glioblastoma Multiforme
Abscess
Intracerebral Hematoma (Subacute)
Cerebral Infarction, Subacute
Radiation Necrosis
Less Common
Tumefactive Demyelinating Lesion
Neurocysticercosis
Lymphoma, Primary CNS
Toxoplasmosis, Acquired
Tuberculoma
Aneurysm (Thrombosed)
Arteriovenous Malformation (Thrombosed)
Ganglioglioma
Pilocytic Astrocytoma
Rare but Important
Lacunar Infarction (Subacute)
Fungal Diseases
Parasites, Miscellaneous
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Solitary ring-enhancing lesions most often related to tumor, infection, or demyelination
Location of lesion often helpful for diagnosis
Metastatic lesions are typically subcortical, while primary tumors are often deep
Smooth rim enhancement suggests abscess
Irregular, thick rim suggests tumor
Helpful Clues for Common Diagnoses
Metastases, Parenchymal
Often significant vasogenic edema
Gray-white matter junction typical
Generally does not restrict on DWI
Multiple > single lesion
Glioblastoma Multiforme
95% of primary GBMs have central necrosis, rim enhancement, DWI negative
Heterogeneous white matter (WM) tumor with irregular, thick rim enhancement
Strong tendency to infiltrate widely
Abscess
Can be pyogenic, fungal, or granulomatous
T2 hypointense rim & thin enhancing rim
DWI + in pyogenic abscess
Look for other signs of infection & source in mastoids & paranasal sinuses
Proton MR spectroscopy (MRS) within pyogenic abscess cavity shows elevated cytosolic amino acids (0.9 ppm), acetate (1.92 ppm), and succinate (2.4 ppm)
Intracerebral Hematoma (Subacute)
History of trauma, coagulopathy, amyloid angiopathy
Ring enhancement common subacutely
Look for blood products on MR (especially on GRE/T2*/SWI sequence)
Cerebral Infarction, Subacute
Signal changes in a vascular territory
May see gyriform T1 hyperintensity
Enhancement: Ring-like &/or gyriform
At this stage, DWI has normalized
Radiation Necrosis
Occurs months after radiotherapy in site of radiation portal
Perfusion MR may discriminate between radiation necrosis & tumor
Radiation necrosis: Hypoperfusion
Tumor: Hyperperfusion
Helpful Clues for Less Common Diagnoses
Tumefactive Demyelinating Lesion
Seen in multiple sclerosis & ADEM
Often incomplete ring enhancement, little mass effect or vasogenic edema; resolves with steroid therapy
Often mimics neoplasm
Neurocysticercosis
Cyst with a scolex is pathognomonic
Ring enhancement seen in colloidal vesicular & granular nodular stage
Lymphoma, Primary CNS
Ring-enhancing pattern seen in immunocompromised patients
Typical locations: Periventricular, corpus callosum, basal ganglia (BG)
Hyperdense on CT, hypointense on T2 MR due to hypercellularity
MRS may differentiate from toxo
Lymphoma: Elevated choline level
Toxoplasmosis, Acquired
Solitary or multiple lesions with nodular or ring enhancement
Occurs in immunocompromised, especially HIV+ patients
Tuberculoma
Associated with TB meningitis in 50%
Can be solitary or multiple
Aneurysm (Thrombosed)
May be partially or completely thrombosed
Laminated appearance of thrombus
May see pulsation artifact on MR
Arteriovenous Malformation (Thrombosed)
May be partially or completely thrombosed
Blood products, calcium are common
Serpiginous nidus seen as flow voids on MR, large draining veins
Ganglioglioma
May be solid, cystic, or mixed solid-cystic
1/3 have calcifications
Temporal lobes & cerebellar hemispheres most common locations
Temporal lobe lesions present with seizures
Pilocytic Astrocytoma
Common locations: Cerebellum, hypothalamus, optic pathway
4 predominant imaging patterns
Mass with enhancing cyst wall & intensely enhancing mural nodule (46%)
Mass with a nonenhancing cyst & intensely enhancing mural nodule (21%)
Necrotic mass with central nonenhancing zone (16%)
Predominantly solid mass with minimal cyst-like component (17%)
Associated with neurofibromatosis type 1
Helpful Clues for Rare Diagnoses
Lacunar Infarction (Subacute)
Typically in BG, thalamus, or deep white matter
May enhance subacutely
Fungal Diseases
Rare infections that occur primarily in immunosuppressed patients
Includes nocardia, blastomycosis, coccidioidomycosis, histoplasmosis, candidiasis
Multiple lesions > single lesion
Parasites, Miscellaneous
Rare infections occur at all ages, most common in children & young adults
Patient’s travel history important
May cause solitary or multiple ring-enhancing lesions
Amebic encephalitis: Single or multiple nodular or ring-enhancing masses
Paragonimiasis: Hemorrhage or infarct with granuloma formation; ring enhancement
SELECTED REFERENCES
1. Smirniotopoulos JG et al: Patterns of contrast enhancement in the brain and meninges. Radiographics. 27(2):525-51, 2007
Image Gallery
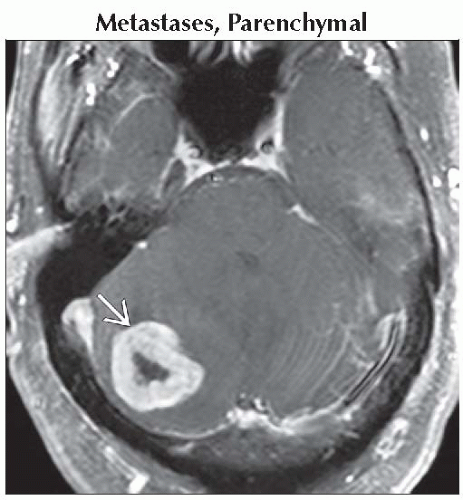 Axial T1 C+ FS MR shows a solitary, thick-walled mass in the right cerebellum  . A thick enhancing rim suggests tumor. Biopsy proved metastatic melanoma. . A thick enhancing rim suggests tumor. Biopsy proved metastatic melanoma. |
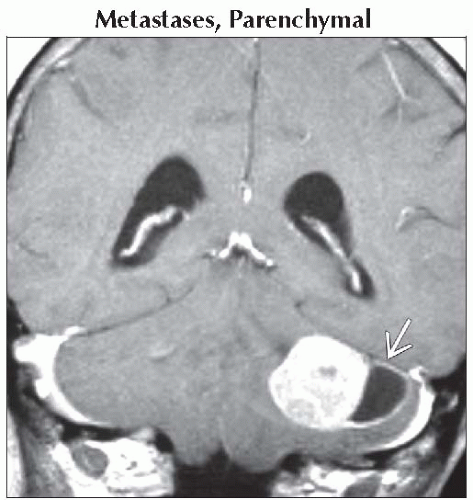 Coronal T1 C+ MR shows a cystic mass with large mural nodule in the cerebellum  . While this lesion resembles hemangioblastoma, the wall of most cystic hemangioblastomas rarely enhances. . While this lesion resembles hemangioblastoma, the wall of most cystic hemangioblastomas rarely enhances. |
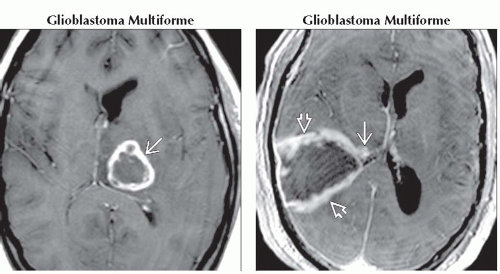 (Left) Axial T1 C+ MR shows a histologically proven glioblastoma multiforme in the left thalamus
 . Note irregular wall & central necrosis. GBMs tend to occur in the deep white matter or deep nuclei & infiltrate widely beyond the enhancing margins. (Right) Axial T1 C+ MR shows a large glioblastoma multiforme . Note irregular wall & central necrosis. GBMs tend to occur in the deep white matter or deep nuclei & infiltrate widely beyond the enhancing margins. (Right) Axial T1 C+ MR shows a large glioblastoma multiforme  with subependymal involvement with subependymal involvement  . Note the irregular peripheral rim enhancement in the tumor. . Note the irregular peripheral rim enhancement in the tumor.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|