Chapter 11 Sacroiliac Joint Block and Neuroablation
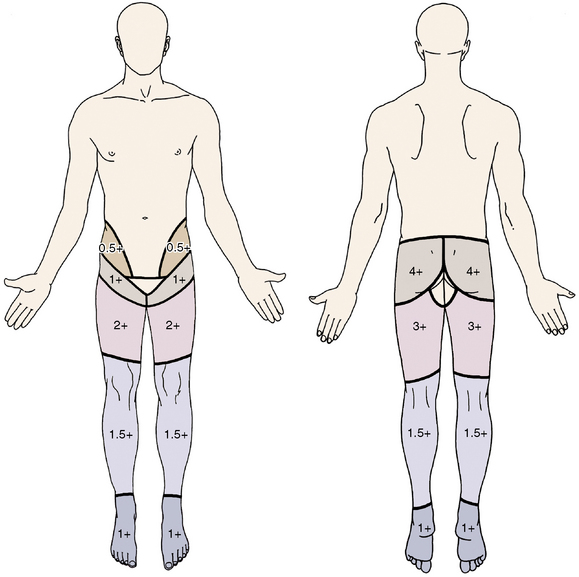
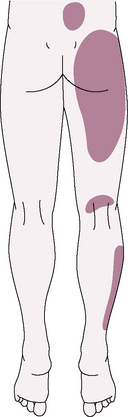
The sacroiliac joint (SIJ) is the largest axial joint in the body with an average surface area of 17.5 cm2 [1]. It is a large, auricular-shaped, diarthrodial synovial joint. However, only the anterior third of the interface between the sacrum and ilium is a true synovial joint; the rest of the junction is comprised of an intricate set of ligamentous connections. If the joints become painful, they may cause pain in the low back, buttocks, abdomen, groin or legs (Figs. 11-1 and 11-2).



Sacroiliac joint dysfunction
Dreyfuss and colleagues [2] have shown that the pain referral pattern in asymptomatic volunteers consists of the following areas:


 Pain in the region of the SIJ with possible radiation to the groin, medial buttocks, and posterior thigh
Pain in the region of the SIJ with possible radiation to the groin, medial buttocks, and posterior thigh


The prevalence of SIJ pain in carefully screened patients with low back pain (LBP) is in the range of 15% to 25%. 39% of patients with SIJ dysfunction were also diagnosed [3] with an associated spinal disorder. Of these spinal disorders complicated by SIJ dysfunction, the most common are as follows:











The following factors predispose an individual to SIJ dysfunction:



The average mechanical threshold of the SIJ nociceptive unit is shown in Table 11.1.
Table 11.1 Average Mechanical Threshold of Sacroiliac Joint and Other Nociceptive Units
| Nociceptive Unit | Average Mechanical Threshold (g) |
|---|---|
| Sacroiliac joint | 70 |
| Lumbar facet joint | 6 |
| Anterior lumbar disc | 241 |


The evidence for the effectiveness of SIJ block and denervation as diagnostic and therapeutic methods for SIJ dysfunction is shown in Table 11.2.
Table 11.2 Level of Evidence for Intra-articular Injection and Neurotomy
| Intra-articular injection: | |
| Diagnostic method | Moderate evidence for diagnosis of pain from the sacroiliac joint (SIJ) |
| Therapeutic method | Moderate evidence for short-term relief (<3 months) Limited evidence for long-term relief |
| Radiofrequency neurotomy | Indeterminate evidence for managing SIJ pain |
Indications






Several major diagnostic tests are used to confirm a diagnosis of intra-articular SIJ pain; they are described in Table 11.3 and Box 11.1, and shown in Figures 11-3 through 11-5.
Table 11.3 Sensitivity and Specificity of Major Diagnostic Tests Used to Identify Patients with Intra-articular Sacroiliac Joint Pain
| Test | Sensitivity | Specificity |
|---|---|---|
| Sacroiliac joint pain | ++++ | + |
| Groin pain | + | +++ |
| Buttock pain | ++++ | + |
| Indication of posterior superior iliac spine as pain source | ++++ | ++ |
| Abnormal sitting posture | + | ++++ |
| Pain lessens with: Nonsteroidal anti-inflammatory drugs Exercise Manipulation | ++ ++ +++ | ++ ++++ ++++ |
| Gillet test | ++ | +++ |
| Patrick test | +++ | + |
| Gaenslen test | +++ | ++ |
| Sacral sulcus tenderness | ++++ | + |
| Midline sacral thrust | +++ | ++ |
| Bone scan | ++ | ++++ |
| Computed tomography | +++ | +++ |
+, 0-25%; ++, 26%-50%; +++, 51%-75%; ++++, 76%-100%.
BOX 11.1 Common Tests Utilized in Evaluation of Sacroiliac Joint Dysfunction
Related posts:
 Atlantooccipital and Atlantoaxial Joint Block for Cervicogenic Headache
Posterior Lumbar Foraminal Decompression
Anterior Endoscopic Cervical Discectomy
Percutaneous Endoscopic Cervical Discectomy and Stabilization
Intervertebral Discography
Transaxial Anterior Lumbar Interbody Fusion Using the AxiaLIF System
Atlantooccipital and Atlantoaxial Joint Block for Cervicogenic Headache
Posterior Lumbar Foraminal Decompression
Anterior Endoscopic Cervical Discectomy
Percutaneous Endoscopic Cervical Discectomy and Stabilization
Intervertebral Discography
Transaxial Anterior Lumbar Interbody Fusion Using the AxiaLIF System
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


