(1)
Princeton Spine & Joint Center, Princeton, NJ, USA
Keywords
Ankylosing spondylitisPregnant womenJoint injectionRadiofrequency rhizotomyThermal barrierIntricate topographySacroiliac joint pain is the third most common cause of chronic lower back pain, accounting for approximately 10–15 % of cases [1]. Recall from chapter one that the sacroiliac joints are the tough, fibrous, stable joints, with some limited but important movement, that translate the forces from the spine to the pelvis and legs. Sacroiliac joint pain is more common in women and also more common in pregnant women and postpartum in particular. In pregnancy, the hormonal changes lead to increased laxity in the ligaments which is what is thought to make sacroiliac joint pain more common in this patient population.
Positions that increase the pressure on the sacroiliac joint naturally tend to exacerbate sacroiliac joint pain. External rotation of the hip such as in sitting cross-legged often irritates sacroiliac joint pain. Sacroiliac joint pain tends to be felt more in the buttocks than in the lower back, per se. Patients with sacroiliac joint pain tend to be able to point more to their pain as it tends to be more focused and less vague. The pain itself is often described as sharper than facet joint pain.
Consider the following patient: Janet is a 32-year-old marketing executive who presents with 6 months of right buttock pain. When asked where the pain is, she points directly to the right buttock over the sacroiliac joint and says that the pain is worse when she does certain yoga poses that involve external rotation of the hip. She says that the pain does not radiate and she denies any neurologic symptoms. The pain is worse when she transitions from sit to stand. On physical examination, her right sacroiliac joint is very tender. She has a positive Patrick’s test in which the left leg is flexed, abducted, externally rotated, and extended and the right buttock pain is reproduced. Her MRI of the LS spine is normal.
Most spine specialists would agree that it sounds like Janet is experiencing sacroiliac joint pain. As with discogenic and facet joint lower back pain, sacroiliac joint pain is ultimately suspected based on history, physical examination, and the presence of relatively benign imaging studies, but it is ultimately diagnosed using fluoroscopically guided diagnostic blocks of the sacroiliac joint [2–5]. Even an X-ray of the sacroiliac joint that reveals sclerosis or fusion may be suggestive of sacroiliac joint pain but is not diagnostic. Dedicated MRI or CT of the sacroiliac joint is rarely performed under normal circumstances because findings on these studies cannot diagnose pain as originating from the sacroiliac joints. X-rays of the sacroiliac joints are generally limited to trying to diagnose or exclude spondyloarthropathies such as ankylosing spondylitis.
While sacroiliac joint pain is generally located in the buttock and is generally confined to the buttock, it may present as pain in the lower back and it has been documented to refer as far down as the foot. Additionally, other causes of chronic lower back pain often present as isolated buttock pain. Therefore, pain located and confined to the buttock suggests sacroiliac joint pain but does not at all confirm it. Reciprocally, lower back pain that refers into the foot at first glance would not appear to be originating from the sacroiliac joint but the diagnosis cannot be excluded and must be considered in the differential diagnosis.
In order to confirm or refute the presence of sacroiliac joint pain, a fluoroscopically guided diagnostic injection of the joint is necessary [6] (Fig. 7.1). When performed, the injection is typically performed with the dual purpose of diagnosis and therapeutics. The anesthetic is the diagnostic piece of the injection. For a few hours after the injection, the pain should be 80–100 % relieved. As with other diagnostic injections, it is important to remember that a person’s pain may be multifactorial. For the diagnostic test to be positive, 80–100 % of one region of the person’s pain should feel better. If a sacroiliac joint injection alleviates the buttock pain but not the lower back pain, then it can be said that the sacroiliac joint is responsible for the buttock pain but not the lower back pain, in which case an alternate diagnosis should be sought for the lower back. All too often, a patient reports that the pain “didn’t get better” when if questioned more carefully, what that patient would say is that one component of the pain was relieved but another piece did not and so overall the patient may not have felt better. If this is the case, it is important to recognize it so that the other components of the pain can be identified and so that the sacroiliac joint is also addressed.
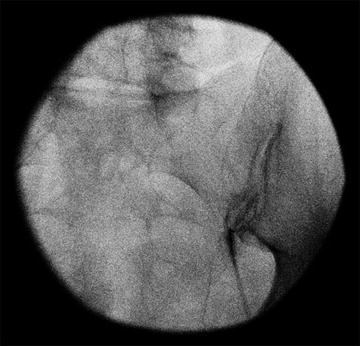
Fig. 7.1
Anteroposterior fluoroscopic image of a right sacroiliac joint injection with contrast enhancement along the joint line
The research on diagnostic blocks of the sacroiliac joint is not as complete as it is with facet joints. Many physicians accept a single positive block as confirmation of sacroiliac joint pain. To approximate a gold standard diagnostic, it would be ideal to block the sacroiliac joint in the same way that the medial branches of the facet joints are blocked to confirm a diagnosis. Ideally, then, the sacroiliac joint would be blocked on at least two separate occasions, once with lidocaine and once with bupivacaine. To be considered positively diagnostic for sacroiliac joint pain, the patient should have longer-acting relief from the bupivacaine than the lidocaine. However, there is a problem with this approach.
When blocking the facet joints, it is the medial branch nerves that are actually blocked. Unlike the facet joints where the medial branch nerves supplying the sensory innervations to the facet joints follow a predictable anatomical path where they can be reliably blocked, the sensory innervations to the sacroiliac joints are numerous, variable, and unpredictable and therefore cannot be diagnostically blocked. Because of this, in order to diagnostically block the sacroiliac joint, the joint itself must be injected. Ropivacaine, mepivacaine, and bupivacaine have all been shown to be chondrocytoxic dependent on the medication, its concentration, and the time of exposure. It is therefore best to avoid these longer-acting anesthetics in intra-articular injections. Because of this consideration most spine specialists block the sacroiliac joint twice as a diagnostic but use lidocaine each time. Further research will hopefully be done to establish a gold standard diagnostic paradigm. In the meantime, the double-block lidocaine paradigm is a generally accepted standard.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


