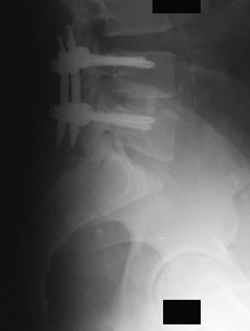
42 A 37-year-old man presented with mechanical back pain after a previous discectomy. On examination, he had decreased sensation in the right L5 dermatome and limited lumbosacral flexion. Preoperative imaging demonstrated a mild disc bulge at L4-L5. Postoperative lumbar spine x-rays (Figs. 42-1 and 42-2) show interbody fusion and percutaneously placed pedicle screws at the L4 and L5 levels. Segmental instability The patient was treated with a percutaneous L4-L5 trans-foraminal lumbar interbody fusion and bilateral L4-L5 pedicle screw fixation and arthrodesis. At follow-up, he was pain free and able to return to work. Mechanical low back pain can sometimes become worse after a decompressive surgery. Segmental instability manifests as axial pain that is worsened by motion and improved by rest, which is typical of mechanical low back pain. There is a differential for failed back syndrome, particularly in the immediate postsurgical period. Low back pain with fever and a reddened wound with discharge are obvious signs of infection. Persistence of a severe radiculopathy may represent a retained disc fragment, incorrect procedural level, or a complex regional pain syndrome. Magnetic resonance imaging (MRI) is an excellent diagnostic aid in these cases and should be done with and without gadolinium.
Segmental Instability
Presentation
Radiologic Findings
Diagnosis
Treatment
Discussion
Segmental Instability
Only gold members can continue reading. Log In or Register to continue







Full access? Get Clinical Tree


