Chapter 13 Seizures and Epilepsy in the Elderly
Introduction
In developed countries, demographic trends project continued increases in the number of older people in the population. In the United States, there were 36.8 million adults over the age of 65 in 2005.1 By 2030, the U.S. Department of Health and Human Services predicts that this figure will have increased to 71.5 million and account for roughly 20% of the population. In this older age group, seizures and epilepsy are the third most common neurological condition, behind only stroke and dementia. Although the primary goals of treatment—freedom from seizures, absence of adverse drug effects, and maintenance of a high quality of life—are the same for all patients with epilepsy, several issues specific to the elderly population need to be considered in approaching diagnosis and making treatment decisions. Diagnosis can be challenging because of the many comorbid conditions that are common in the elderly. These comorbidities, along with the medications prescribed to treat them, must be considered carefully when devising treatment strategies. Dealing with these issues will only become more challenging in the coming years, as the number of people over the age of 65 increases steadily.
Epidemiology
The incidence of both acute symptomatic seizures and unprovoked seizures or epilepsy is highest in people over the age of 65.2–4 In a British population study, nearly 25% of newly identified seizures occurred in patients 60 years of age or older.5 The incidence continues to rise with increasing age: In those older than 75, the incidence is five times that of younger adults. In the United States, about 50,000 new cases of epilepsy occur each year in this age group.6
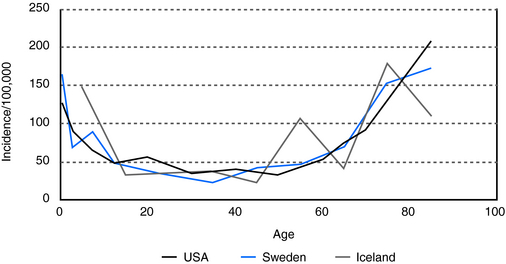
In people over 60 years of age, the prevalence of unprovoked seizures and epilepsy is at least 1%, and it is even higher, 1.2 to 1.5%, in people over 75 (Figure 13-1). This is a prevalence rate about twice that seen in younger adults.10,11 In a study of 1, 130, 155 U.S. veterans who were at least 65 years of age, 1.8% had epilepsy.12,13 In specific populations at risk, such as nursing home residents, who have significantly higher rates of comorbid conditions associated with epilepsy, including dementia and stroke, prevalence rates as high as 3 to 9% have been reported.14–16
Etiology
ACUTE SYMPTOMATIC SEIZURES
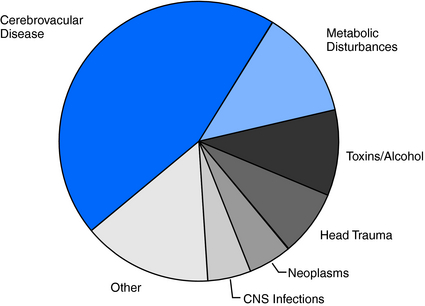
Because brain injuries caused by stroke, head injury, infections, neoplasms, and metabolic disturbances (hypoglycemia, hyponatremia, uremia) are so common in the elderly, it is not surprising that the incidence of acute symptomatic seizures is likewise high in this age group.6 Cerebrovascular disease accounts for 40% to 50% of acute symptomatic seizures, metabolic disturbances for 10 to 15%, and acute head trauma, brain infections, neoplasms and toxins/alcohol each for 5 to 10%2,6,17 (Figure 13-2).
UNPROVOKED SEIZURES AND EPILEPSY
The high frequency of unprovoked seizures and epilepsy in elderly persons can also be attributed in large part to the high prevalence of a history of stroke, brain tumor, and head trauma in older age groups. Even so, about 50% of cases remain cryptogenic (Figure 13-3), although this is a significantly lower percentage than that found in younger age groups, where about 70% of cases have no identifiable cause.3,17
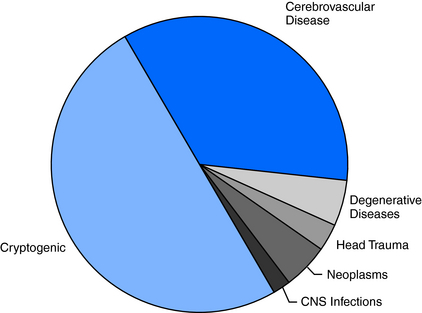
Cerebrovascular disease is the most frequently identified antecedent of epilepsy, accounting for 30 to 40% of all new cases.6,18 Individuals with cerebrovascular disease are 20 times more likely to develop epilepsy than the general population.19 About 15% of stroke survivors will develop unprovoked seizures within the first 5 years, and the elevated risk continues for many years thereafter.
Seizures may, in fact, be the first presentation of unrecognized cerebrovascular disease. This is especially true if previous strokes had occurred in clinically silent brain areas. In a review of new onset seizures in 4709 patients older than age 60, none of whom had a known history of cerebrovascular disease, dementia, tumor, or alcohol abuse, Cleary and colleagues found that the relative risk of stroke was nearly three times that of controls.20 Hypertension is also an independent risk factor for unprovoked seizures,21 although hypertension may be a surrogate for the progressive arterial changes associated with lacunes, other small strokes, and periventricular white matter lesions.
Although the incidence of head trauma is highest in adolescents and young adults, a relative peak of occurrence in the elderly is largely attributable to falls. Approximately one-third of people over the age of 65 living at home, and about half of nursing home residents, have at least one fall each year.22,23 Trauma with loss of consciousness is associated with a threefold increased risk of epilepsy.6 With more severe head injuries, risk is even higher. Overall, head trauma accounts for 2 to 3% of new cases of epilepsy in the elderly.
Although the incidence of central nervous system infections is highest in childhood, a second peak occurs in the elderly. Survivors of central nervous system (CNS) infections have a threefold risk of developing epilepsy, and a history of infections accounts for 2 to 3% of cases.24
Alzheimer’s and other neurodegenerative diseases are associated with a 5- to 10-fold increase in epilepsy compared to the general population.6,25 Unprovoked seizures may be seen in as many as 8 to 15% of patients with Alzheimer’s disease.25,26
Clinical Presentation
As would be expected from the etiological profile, the great majority of seizures in the elderly, more than 70%, are of partial onset.18,27,28 Even generalized tonic-clonic seizures without obvious focal features are likely to have a localized or regional onset, as it is very unusual for idiopathic generalized epilepsy syndromes to present at this age. In any event, diagnosis of epilepsy in the elderly can be difficult and may be delayed. In a recent Veteran’s Administration cooperative study of epilepsy in elderly patients, epilepsy was an initial diagnostic consideration in 73% of patients that were eventually diagnosed with epilepsy.18 In a subset of 151 patients from this study, Spitz and colleagues found that the delay from initial symptoms to diagnosis was 2.3 years, with a median time of 1 year. Only 37% of patients in this subgroup were correctly diagnosed at the time of initial evaluation. Two-thirds of patients with generalized tonic-clonic (GTC) seizures, but only one-fourth of patients with complex partial seizures, were correctly diagnosed.29
Because the lesions associated with epilepsy in elderly people can involve any area of the brain, extratemporal neocortical epilepsies are more common than in younger adults. Consequently, seizures may manifest with a wide variety of sensory, visual, cognitive, and behavioral phenomena that are frequently atypical for the physician’s experience and thus more difficult to recognize as having an epileptic basis. Classic auras are less common in the elderly, and initial manifestations of partial seizures, such as dizziness, a vague feeling related to the head, memory loss, or confusion, may be interpreted as nonspecific symptoms due to any number of possible causes. Thus, given the high frequency with which metabolic derangements, cerebrovascular events, and dementia occur in the elderly, clinical manifestation of partial seizures, as well as of postictal states, may be incorrectly attributed to these other conditions. For example, postical aphasia or hemiparesis may be diagnosed as ischemic events.30 Finally, although published data are lacking, it is said that generalized tonic-clonic seizures, the easiest type of seizure to recognize, occur with less frequency in older age groups.
Falls in the elderly are common and a frequent cause of admission to a hospital.23 However, seizures are rarely considered an important etiology, especially early in the diagnostic evaluation. More often, falls are attributed to cardiovascular, cerebrovascular, or arthritic etiologies. Confusion or memory loss, which may be ictal or postical in nature, is often first considered to be a manifestation of dementia, metabolic abnormalities (e.g., dehydration) or a head injury related to a fall.
Difficulty in diagnosis is compounded by the increase in social isolation in the elderly population. In 2006, the U.S. Department of Health and Human Services found that 30% of noninstitutionalized people over 65 years of age, totaling more than 10 million people, lived alone.1 As such, elderly patients are often brought to the hospital by emergency medical services without anyone available to provide information through direct observation of an episode.
NONEPILEPTIC PAROXYSMAL PHENOMENA
As at other ages, elderly persons can have episodic paroxysmal phenomena that mimic seizures but are nonepileptic (Table 13-1). In a study of 94 patients at least 60 years of age (mean 70 years) who were referred for video-electroencephalogram (EEG) monitoring for evaluation of paroxysmal episodes, 27 (29%) had nonepileptic events, including 13 with psychogenic seizures.31 The majority of these patients had been taking antiepileptic drugs for presumed epileptic seizures. Such findings underscore the need for video-EEG monitoring in patients whose seizures are atypical or have not responded to treatment with antiepileptic drugs (AEDs).
TABLE 13–1 Paroxysmal Phenomena That May Mimic Seizures in Elderly Patients
| Syncope |
| Transient ischemic attacks |
| Transient global amnesia |
| Migraine |
| Drop attacks |
| Myoclonus |
| Confusional episodes due to medication interactions or overmedication |
| Hypoglycemia |
| Electrolyte disturbances/dehydration |
| REM behavior disorder |
| Nonepileptic psychogenic seizures |
Risk of Recurrence
Physicians should have a low threshold for suspecting seizures in the elderly because of the increased incidence and the higher rate of seizure recurrence in this population.3,4
In patients presenting with a first unprovoked seizure, the overall risk of recurrence with at least 2 years of follow-up is about 38% (range 25 to 52%).32–35 Factors that increase the risk of recurrence include abnormal EEG findings and presence of an underlying definable etiology.
Data regarding specific effects of older age on risk of recurrence are inconclusive, and there are no population-based studies. However, when seizures can be attributed to a recognized underlying neurologic condition (that is, they are symptomatic of an acquired pathogenic mechanism), risk of recurrence is roughly double that of a cryptogenic first seizure.33 In selected populations, the recurrence rate may be especially high. For example, seizures recurred in more than 80% of a small series of patients with a remote history of stroke.36
Treatment Considerations
Although it often stated that epilepsy is more easily controlled in elderly patients than in younger ones,37,38 it is not clear that this is accurate, as no well-controlled large studies specifically address this issue. Data from two recent studies looking at tolerability of anticonvulsant drugs in the elderly showed that seizure-free rates are similar to those seen in the adult population at large. In a randomized trial that compared response in the elderly to treatment regimens using modest dosages of carbamazepine (dosage range 200 to 800 mg daily) and lamotrigine (dosage range 75 to 300 mg daily), Brodie and colleagues found that only 33% remained seizure free during the final 16 weeks of the study.39 Although a high rate of medication withdrawal likely contributed to the relatively low rate of seizure control, these findings suggest that seizures are, in fact, not necessarily easily controlled in this population. Similarly, in the VA cooperative study #428, which randomized elderly patients with new-onset epilepsy to treatment with gabapentin, lamotrigine, or carbamazepine, 53% of patients who remained on treatment were seizure free at 12 months.40 These data are not substantially different from seizure control rates in the general population, as illustrated by the study by Kwan and Brodie of 470 previously untreated patients with epilepsy, ranging in age from 9 to 93.41 They found that 47% of patients became seizure free on the first drug, and a total of 61% became seizure free with the second or third monotherapy agent.
PHARMACOKINETIC CHANGES
Absorption
Absorption of drugs depends on dissolution of their particular formulations. This, in turn, is mainly related to gastric acid secretion, which often declines in the elderly.42 In addition, to varying degrees, gastric emptying slows, intestinal transit time increases, mesenteric blood flow decreases, and the intestinal absorptive surface may decrease.43 All these changes contribute to variable and often unpredictable absorption of different drugs. Overall, this combination of factors typically results in a diminished ability to absorb antiepileptic drugs, which reduces their bioavailability.
These age-related changes in absorption can be compounded by frequent use of antacids, which can specifically impair absorption of phenytoin. In addition, gabapentin, which is absorbed via a saturable L-amino acid transporter system in the small intestine,44 may be particularly susceptible to physiological changes in gastrointestinal absorption.
Protein Binding
In healthy adults, serum albumin concentration decreases only slightly with age.45 However, in elderly patients with acute systemic and neurological illnesses, serum albumin levels can decline significantly. Suboptimal nutrition may exacerbate this. With reductions in serum albumin concentrations, the free fraction of highly protein-bound medications can increase substantially, sometimes resulting in prominent adverse effects despite little or no change in the total serum level.
AEDS that are highly protein bound include tiagabine, phenytoin, valproate, diazepam, clonazepam, clobazam, and to a lesser extent, carbamazepine.46
Related posts:
 The Life-Threatening Epilepsies of Childhood and Their Treatment
The Life-Threatening Epilepsies of Childhood and Their Treatment
 The Spectrum of Epilepsies Associated with Generalized Spike-and-Wave Patterns
The Spectrum of Epilepsies Associated with Generalized Spike-and-Wave Patterns
 Epilepsies Due to Monogenic Disorders of Metabolism
Epilepsies Due to Monogenic Disorders of Metabolism
 The Surgery of Temporal Lobe Epilepsy I—Historical Development, Patient Selection, and Seizure Outcome
The Surgery of Temporal Lobe Epilepsy I—Historical Development, Patient Selection, and Seizure Outcome
 Cortical Myoclonus and Epilepsy: Overlap and Differences
Cortical Myoclonus and Epilepsy: Overlap and Differences
 Does Early Treatment Influence the Long-Term Outcome of Epilepsy?
Does Early Treatment Influence the Long-Term Outcome of Epilepsy?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


