Aura: First part of sz, often the only part remembered by pt; a focal sz that sometimes progresses to focal dyscognitive or secondarily generalized sz.
Postictal period: The period from end of sz until return to baseline.
Epilepsy: ≥2 unprovoked szs ≥24 h apart, or a tendency toward recurrent unprovoked szs.
Epilepsy syndrome: Specific form of epilepsy; implies specific cause, si/sx, prognosis.
Status epilepticus (SE): Continuous sz lasting >5 min or >1 sz w/o full return to baseline.
Epidemiology of epilepsy (NEJM 2008;359(2):166): 45 M cases worldwide; USA ˜7/1,000; 70% focal, 30% generalized. Causes (adults): 60% unk; 40% known causes—stroke 9%, TBI 9%, EtOH 6%, neurodegen 4%, static encephalopathy 3.5%, brain tumor 3%, infxn 2%.
DIFFERENTIAL DIAGNOSIS OF SEIZURES
(Adapted from https://www.epilepsydiagnosis.org/epilepsy-imitators.html)
Syncope (including “convulsive syncope,” see below): Vasovagal, orthostatic, long QT/cardiogenic, breath-holding spells.
Transient ischemic attack: Usually presents w/(-) sxs, but can have (+) sxs (e.g., jerking, rigidity, hallucinations, visual illusions). Limb-shaking TIA a/w preocclusive carotid disease. Todd paralysis (transient weakness after sz) can mimic TIA/stroke.
Transient global amnesia:Dx: Acute-onset anterograde amnesia; no &Dgr; consciousness/loss of self-awareness; cog. impairment ltd to amnesia; no recent TBI or sz; sx duration <24 h; & no other neuro sx other than dizziness, vertigo, HA. Workup: MRI may show punctate DWI bright lesion in the hippocampus, usu 24-48 h after sx onset. If atypical presentation or signif vascular risk factors consider stroke w/u. Etiology/prognosis: Etiology unknown (theories: venous congestion, hippocampal TIA). Prognosis: Usu benign, not recurrent.
APPROACH TO THE PATIENT WITH TRANSIENT LOSS OF CONSCIOUSNESS
HPI: Hx key for dx. (J Neurol 2009;256:155-167). These features suggest but not definitive for dx. Abbreviations: OS, orthostatic; VV, vasovagal; CG, cardiogenic; HV, hypovolemic.
During spell:Fall: flaccid → syncope(any), stiff → sz. Movements: symmetric, synchronous, focal, prior or at onset of LOC → sz; nonrhythmic, multifocal, small amplitude, <15 s, always after LOC → syncope(any). Eyes: gaze deviation → sz; open → sz & syncope(any); closed → PNES. Tongue biting: lateral → sz (40% of GTCs); tip of tongue → syncope(any, in 2%-6%). Skin: cyanotic → sz; pale → syncope(any). Others: head turn to one side → sz; mouth frothing → sz; incontinence → sz or syncope(any); preserved awareness → PNES.
After spell: Consciousness: prompt recovery (<1 min) → syncope, psychogenic; postictal confusion (minute to hours) → sz. Others: HA, muscle ache → sz; Todd paralysis → sz; emotional lability → psychogenic.
Exam: (1) VS ✓ orthostasis: supine to standing → >20 mm Hg ↓ SBP, >10 mm Hg ↓ DBP, or >10-20 bpm ↑ HR. (2) HEENT: E/o head trauma, tongue laceration. (3) CV: murmurs, rhythm, HF (↑ JVP, S3, displ PMI), carotid bruits. (4) Neuro: mental status, focal deficits.
Initial workup: EKG, CBC, chem7, serum & urine tox screen; young women ✓pregnancy.
If HPI suggests syncope (and initial w/u neg), consider (1) echo: r/o structural heart dz; (2) exercise stress test: esp w/exertional syncope; (3) tilt table (provokes vasovagal syncope): (+) in 50% w/recurrent unexplained syncope; Se 26%-80%, Sp >90%; (4) Holter or loop monitor; (5) referral to cardiology.
If HPI suggestive of sz: Imaging (CT/MRI brain), EEG, sz w/u (see below).
If HPI suggestive of psychogenic nonepileptic szs, see below.
Treatment of syncope: (1) HV: rehydrate acutely, encourage regular fluid intake. (2) OS (autonomic dysfxn): advise to rise slowly, use compressive stockings, increase fluids, & ↑ Na diet. If conservative measures fail, consider midodrine, fludrocortisone, anticholinesterases. (3) VV: identify & avoid triggers. No proven benefit w/&bgr;-blockers (Circulation 2006;113;1164). (4) CG: depends on etiology, consider ref to cardiology & adjustment of vasoactive meds.
PSEUDOSEIZURES (PSYCHOGENIC NONEPILEPTIC SZS, PNES, OR NES)
Def: Spells resembling epileptic szs but w/o EEG correlate. Psych origin; usu somatoform (conversion > somatization> > factitious, malingering). ˜30% PNES pts also have epileptic szs.
HPI suggestive of PNES: Multiple nl EEGs, no response to AEDs, strange triggers (stress, pain, specific mvmts, sounds, lights), occur only around others (e.g., doctor’s office), florid ROS, vague somatic sxs, inappropriate lack of concern (“la belle indifference”), inducibility by suggestion, h/o sexual trauma, fibromyalgia, chronic pain, fatigue, depression, anxiety.
Semiology suggestive of PNES vs. seizure: See table.
Dx: Difficult by hx/exam alone. Provocation (suggestion, hyperventilation, photic stim, saline injection), useful, but ?ethical. Gold std: video EEG showing nl EEG during stereotyped event (though EEG can be falsely nl w/deep or midline sz). EEG helps distinguish epileptic vs. NES in pts w/both. May need to capture multiple events before definitive dx of PNES.
Prognosis: Generally poor, but better outcomes assoc w/young onset, early dx, less dramatic features, no other somatoform c/o; hypomotor features (vs. thrashing). In kids w/PNES: Suspect ongoing sexual abuse, mood d/o (Epilepsia 2012;53(10):1679-1689).
Signs: PNES vs. Seizure
PNES
Seizure
Se
Sp
Se
Sp
Preserved awareness
56%
93%
Eyes open/widen
100%
84%
Eye flutter
50%
>95%
Abrupt onset
94%
55%
Others alleviate/intensify
55%
>95%
Postictal confusion/sleep
81%
70%
Postictal whispering
58%
83%
Eyes fixed
57%
92%
Stuttering course
42%
>95%
Clenched mouth
9%
92%
Forced eye closure
33%
>95%
Hand automatisms
26%
>95%
Pelvic thrusting
8%
>95%
Ictal scream
22%
>95%
Arched back
8%
>95%
Grasping
9%
>95%
Head side to side
25%
87%
Postictal nose wiping
23%
>95%
Ictal crying
8%
91%
Postictal aphasia
9%
>95%
Turn onto belly
<5%
87%
Postictal snoring
35%
>95%
Ictal whispering
58%
78%
Abrupt offset
75%
70%
Immediate return to b/l
64%
55%
Onset in single limb
57%
67%
Nonsynchronous mvmt
17%
78%
Eyes rolled back
52%
67%
Seizure >2 min
67%
48%
Aura
50%
17%
Se, sensitivity; Sp, specificity; b/l, baseline; mvmt, movements.
Adapted from Ann Neurol 2011;69:997.
EVALUATION OF PATIENTS WITH SEIZURE
Clinical eval: HPI: Provoked vs. unprovoked? (see table below). Preceding illness/fever, trauma; aura, ictal/postictal si/sx (confusion, depression, aphasia, exhaustion, sleep, fear, HA, amnesia, nausea, pain, perceptual distortions, psychosis, thirst, wkns).
PMH/ROS: Epilepsy risk factors: FHx sz, early hx (prenatal, birth, perinatal), febrile sz, delay in developmental milestones, birthmarks/congenital anomalies, prior szs, stroke, head trauma, CNS infxns. Sz hx: Semiology (best directly from witness), diurnal variation, relation to menses, myoclonic jerks, photosensitivity, injuries during sz, # of ED visits for sz in past yr, prior AEDs & why d/c’d. Triggers: AED noncompliance, sleep deprivation, EtOH use, stress, flashing lights, fever, menses. Prior studies: EEG, CT, MRI, PET, SPECT.
Exam: Gen: Skin exam for neurocutaneous d/os (e.g., café au lait, ash leaf macules), body asymmetry, head circumference. Neuro: Focal abnlities (suggestive of underlying cause).
Tests: Standard w/u: (1)Labs: CBC, chem7, LFTs, Stox, Utox, AED levels, UA, CXR. (2)Imaging: CT if urgent (if concern for acute stroke, ICH, large mass). MRI ± gado preferable (structural abnls: tumor, stroke, infxn, AVM), w/coronal T2 (assess hippocampus). (3) EEG (see below). Consider further w/u: LP if suspected meningitis/encephalitis, SAH, all HIV+ pts.
Prediction of seizure recurrence: Incidence of 2nd sz in adults ˜40%-50% w/in 2 yr (Neurology 1991;41:965; Neurology 1993;43:478; Lancet 2005;365:2007). Yield of EEG ↑ w/in 24 h of sz, 51% vs. 34% when done later (Lancet 1998;352:1007). If 1st EEG nl, sleep-deprived EEG can ↑ likelihood of finding epileptiform abnlities. Multicenter Epilepsy & Single Sz (MESS) study: Neuro exam, imaging, & EEG all nl → “low” risk (30%) of recurrence w/in 5 yr; 1 of above abnl = mod risk (50)%; 2 abnl = high risk (70%) (Lancet Neurol 2006;5:317). AEDs: After 1 unprovoked definite sz: if nl neuro exam, nl imaging, & nl EEG → OK to defer tx; if abnl exam, imaging, EEG or ≥2 szs → start AED.
Etiology of Provoked Seizures
Primary neurologic d/os
Acute/subacute neurologic insult: Head trauma, meningitis/encephalitis, brain abscess, stroke, SAH, HIV encephalopathy, cerebral anoxia, hypertensive encephalopathy/PRES, eclampsia, neurosurgery
Structural abnlities: Mass lesions, vascular malformations
(1) How to keep a pt safe during a sz: (1) Stay calm. (2) Time the sz. (3) Turn pt on side to prevent choking. (4) Loosen tight clothing & place something soft under the head. (5) Don’t put anything in pt’s mouth. (6) Don’t restrain pt. (7) Call 911 if sz lasts >5 min or pt has >1 sz w/o return to baseline. (8) Stay w/pt until awake/alert, or until medical personnel arrive. (2) General safety: Szs can result in signif bodily harm & death. Common sense: Don’t swim/bathe alone; avoid heights & tall ladders; avoid power tools, heavy machinery, welding equipment; avoid high-risk sports (e.g., scuba diving, hang gliding, motor sports, boxing, downhill skiing, long-distance swimming, hockey). (3) Driving: Pts w/epilepsy account for 0.02%-0.04% of all reported motor vehicle accidents (in comparison, 7% of motor vehicle accidents are EtOH related). Laws for resuming driving vary by state. State-specific regulations: http://www.epilepsy.com/driving-laws. Some make allowances for purely nocturnal szs & pts w/consistent pattern of prolonged aura (Epilepsia 1994;35:662-705). (4) AED compliance, side effects, drug interactions. Refer to AED section for specific AEDs. Pts taking enzyme-inducing AEDs should take Ca 1,200 mg qd + VitD 2,000 IU qd & receive routine osteoporosis screening. (5) Depression screen: W/controlled epilepsy, prevalence = 10%-30%; w/refractory epilepsy = 30%-50%; & gen’l pop’n = 5%-17%. Lifetime prevalence of suicidal ideation in epilepsy (4.6%-30%) 2× c/w gen’l pop’n (1%-7%). (6) Women’s issues: See also Pregnancy Neurology chapter. Discuss contraception, family planning, pregnancy. All women of childbearing age should take folic acid (0.4-0.8 mg qd), prior to conception & during pregnancy (Wyllie’s Treatment of Epilepsy. 5th ed., Chapters 93-95).
STATUS EPILEPTICUS (SE)
Practical def: Sz >5 min or >1 sz w/o return to baseline b/w szs (failure of spontaneous sz termination). Focal or generalized, convulsive (CSE) or nonconvulsive (NCSE).
Related Dxs: (1) Sz clusters: Return to baseline b/w szs (less urgent than SE, but ↑ risk of SE). If at home w/sz clusters or prolonged sz, Rx w/rectal diazepam gel (Diastat) 0.2 mg/kg, OR SL lorazepam 1 mg, OR nasal midazolam 0.1-0.2 mg/kg; call EMS. (2) NES: May be difficult to distinguish; clues favoring szs: hypoxemia, ↑ CPK, acidosis.
Etiologies of SE (most to least common): Adults: ↓ AED levels, stroke, remote TBI/congenital malf., EtOH w/d, anoxic injury, metabolic disturbance, drug intox’n, CNS infxn, brain neoplasm, idiopathic, acute TBI. Kids: Febrile szs, remote TBI/congenital malf., ↓ AED levels, acute TBI, stroke, drug intox’n, anoxic injury, metabolic disturbance, CNS infxn, idiopathic.
GENERALIZED CONVULSIVE STATUS EPILEPTICUS (GCSE)
Generalized convulsions, most often tonic-clonic but can also be myoclonic, tonic, or clonic. As GCSE progresses, motor activity ↓ amplitude & later ceases; 48% pts w/GCSE → nonconvulsive szs (NCS) w/in 24 h; 14% have NCSE. If LOC fails to improve by 20-30 min after convulsions → high probability for NCSE; obtain urgent EEG to confirm & manage.
Epidemiology: Incidence in the United States 20-40/100 k. Bimodal distribution across the life span, most common in kids <1 yo & adults >60 yo. 50% of pts w/GCSE have acute neurologic injury, & >50% never had a prior sz. 15% pts w/epilepsy have at least one episode of SE.
Physiologic complications:Neurologic injury: Glutamate-mediated excitotoxic injury. Szs create ↑ metabolic demand, requiring ↑ cerebral blood flow. Failure of cerebral autoregulation leads to ↑ cerebral edema, ↑ ICP, ↓ cerebral perfusion. Systemic disturbances: Hypoxia, hypercapnia, aspiration PNA, pulmonary edema, HoTN, cardiac arrhythmia, cardiac injury, rhabdomyolysis, ATN, hyperthermia, metabolic disturbances (glucose, K, Na, phos, pH). EEG: Five stages: (1) Discrete szs. (2) Merging of discrete szs. (3) Continuous ictal discharges. (4) Continuous ictal activity punctuated by flat periods. (5) Periodic epileptiform discharges. Imaging: Brain MRI superior to head CT. Transient MRI &Dgr;s include DWI &Dgr;s or ↑ FLAIR in hippocampus, neocortex, corpus callosum, posterior thalamus. Treatment: Early tx a/w better outcomes. EEG NOT required for dx of GCSE, should NOT delay tx. Use pre-established time-based algorithm (e.g., table below). Prognosis: M&M vary w/age, etiology, duration. Mortality predictors: Older age (mortality in kids ˜3%; adults <60 yo ˜26%; >60 yo ˜39%; >80 yo ˜50%); longer duration (mortality in SE lasting <1 h ˜3%, >1 h ˜32%); etiology (highest mortality: anoxic brain injury). Twenty to fifty percent of survivors have significant functional disability. Status Epilepticus Severity Score (STESS; see table) somewhat predicts survival.
Status Epilepticus Severity Score (Neurology 2006;66:1736; J Neurol 2008;255(10):1561-1566)
Features (determined prior to treatment initiation)
Score
Level of consciousness
Alert or somnolent/confused Stuporous or comatose
0
1
Worst seizure type
Simple partial, complex partial, or absence Generalized convulsive
Nonconvulsive status epilepticus in coma
0
1
2
Age
<65 yr
≥65 yr
0
2
Hx of previous seizures
Yes
No or unknown
0
1
Total
0-6
Scores of 0-2 have favorable prognosis (97% survive; of survivors, 81% return to clinical baseline). Scores ≥3 do not accurately predict mortality & should not be used to justify withdrawal of care.
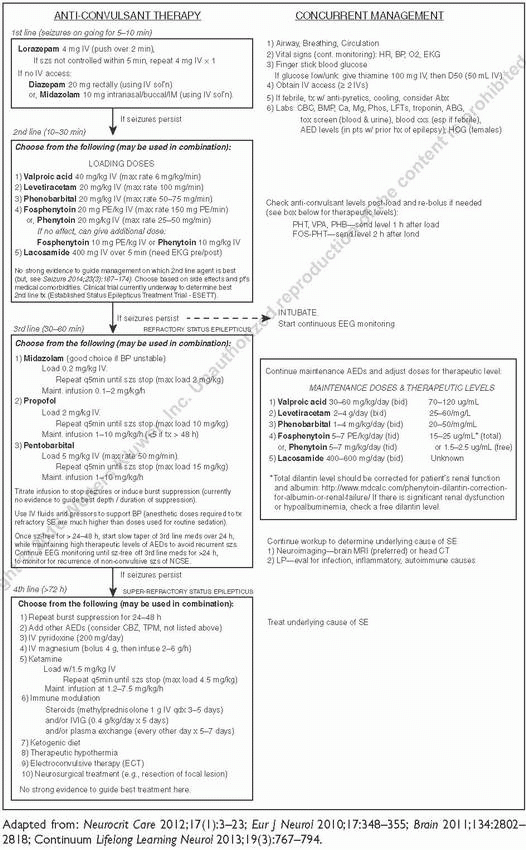
TREATMENT PROTOCOL FOR GCSE
NONCONVULSIVE STATUS EPILEPTICUS (NCSE) (AKA ELECTROGRAPHIC SE, ESE)
Def: SE w/o evident convulsions, often p/w AMS (confusion to coma) w/absent/minor motor si/sx. Can be primary or follow GCSE. P/w: Agitation, amnesia, aphasia, catatonia, confusion, echolalia, laughter, lethargy, perseveration, personality &Dgr;, psychosis, singing, automatisms, eye blinking/deviation, face/finger twitching, nystagmus, tremulousness.
Epidemiology: In pts w/unexplained altered consciousness, 18% had nonconvulsive szs (NCS), 10% in NCSE, ˜75% of szs in the critically ill are NCS. In pts with unexplained coma & no prior szs, 8% were in NCSE. In neuro-ICU pts, electrographic szs found in 27%-34%. Risk factors: Critically ill, ICH, CNS infxn, epilepsy, severe AMS, oculomotor abnls, periodic discharges, or suppression burst on EEG (Clin Neurophysiol 2007;188:1661).
How long to monitor on EEG: Risk stratified based on presence of epileptiform discharges (ED), incl spikes, sharps, periodic discharges, triphasic waves. Pts w/ED: probability of sz w/in 72 h is <10% & <5% if sz-free >7 & 16 h, resp. Pts w/o ED: probability of sz w/in 72 h <10% & <5% if sz-free for 15 min & 2 h, resp (Clin Neurophysiol 2014;126:463).
Diagnosis
1. NCSE by strict electrographic criteria: requires EEG (see table below for criteria)
2. NCSE by electroclinical criteria: EEG shows a rhythmic/periodic pattern that does not meet criteria as below but clearly correlates with si/sx.
3. NCSE by electroradiologic criteria: EEG shows a rhythmic/periodic pattern that does not meet criteria as below but clearly correlates with brain imaging (MRI, PET) findings.
Treatment: No strong evidence to guide tx; decision must be made on case-by-case basis, weighing potential benefits of aggressive tx (e.g., intubation, high dose anesthetics) vs. potential risks. Benefits: Rapid termination of szs, prevention of sz-induced secondary brain injury. Risks: Side effects of anesthetics (e.g., hypotension, propofol infusion syndrome), prolonged mechanical ventilation & ICU course, with attendant risks of infection.
Prognosis: Status Epilepticus Severity Score (STESS, see table) predicts survival. NCSE in coma portends poorer prognosis. NCSE after GCSE has 2× mortality c/w GCSE alone.
Criteria for Nonconvulsive Seizure
EEG pattern = nonconvulsive sz, if duration >10 s & ≥1, primary criteria met. Primary criteria
1.
Repetitive generalized or focal spikes, sharp waves, spike-&-wave, or sharp-&-slow wave complexes at ≥3 Hz.
2.
Same as above but frequency <3 Hz + satisfies the secondary criterion (below).
3.
Sequential rhythmic, periodic, or quasiperiodic waves at ≥1 Hz & unequivocal evolution in frequency (gradually ↑ or ↓ by at least 1 Hz), morphology, or location (gradual spread into or out of a region involving >1 electrodes). Amplitude evolution alone is insufficient.
Secondary criterion
1.
Positive response to trial of rapidly acting AED, e.g., benzo. (see next table).
J Clin Neurophys 2005;22(2):79-91.
Benzodiazepine Trial for Dx of NCSE (Clin Neurophys 2007;118(8):1660-1670)
Benzo trial: Sequential doses of rapidly acting short-duration BZD, e.g., midazolam at 1 mg/dose. Between doses, repeated clinical & EEG assessment. Trial is stopped after any of the following: (1) Persistent resolution of the EEG pattern (& exam repeated). (2) Definite clinical improvement. (3) Respiratory depression, hypotension, or other adverse effect. (4) Maximum allowed dose is reached (e.g., 0.2 mg/kg midazolam).
Test is (+) if ictal EEG pattern resolves & EITHER improvement in clinical state OR appearance of previously absent nl EEG patterns (e.g., posterior “alpha” rhythm). Test is equivocal if EEG improves but pt does not.
NEW-ONSET REFRACTORY STATUS EPILEPTICUS (NORSE)
Pts (often young, healthy) p/w refractory SE a/w cryptogenic encephalitis-like illness. Related dxs in kids: idiopathic hemiconvulsion-hemiplegia & epilepsy syndrome (IHHES), febrile infection-related epilepsy syndrome (FIRES). Natural hx: Prodrome: Low-grade fever, flulike illness, mild resp, or GI infxn. Early phase: Discrete szs, encephalopathy, focal deficits. Fulminant phase: Refractory szs & SE, up to 30% mortality. Remission: SE controlled. Chronic: Often poor functional outcome, w/refractory epilepsy, cognitive impairment, brain atrophy. Etiology: Unk/varies; causes incl unidentified infxn, parainfxn, inflammatory, autoimmune. Workup: Identify treatable dzs (infxn, autoimmune, paraneoplastic). MRI of the brain (acute brain injury, limbic encephalitis, encephalomyelitis), CSF (r/o infxn, send auto-Abs), EEG to guide tx of SE/nonconvulsive szs. Tx: Tx underlying cause if found (infxn, abx/antivirals; paraneoplastic, find/tx tumor; autoimmune, immune therapy). For szs/SE: Follow SE protocol above (Ann Acad Med Singapore 2005;34:417-20; Epilepsia 2010;51(7):1323-1328).
General principles: Prognosis & optimal tx depend on characterization of sz type & epilepsy syndrome. Appropriate level of detail in characterization varies w/clinical situation.
2010 ILAE classification of clinical seizures & epilepsy (Epilepsia 2010;51:676): Generalized sz: Sz that rapidly engages bilateral networks.
Focal sz: Sz that originates w/in networks limited to one hemisphere; described by clinical features (see tables below) & whether consciousness is impaired (focal dyscognitive sz). Terms complex partial & simple partial no longer in the ILAE classification, though still widely used in clinical practice.
Unknown sz: Cannot clearly be categorized as generalized or focal (e.g., epileptic spasms).
Epilepsy Etiologies (not exhaustive; see Epilepsia 2001;42:796-803)
Generalized rapid jerks of limbs, consciousness usually intact Dur: <1-2 s; LOC+, PC-
Gen’d polyspike & wave
Atonic
Myoclonic sz followed by atonic sz Dur: 5-10 s; LOC±, PC±
Tonic
Myoclonic sz followed by tonic sz Dur: 5-20 s; LOC+, PC±
Focal
Depends on localization, may have motor, sensory, experiential, dyscognitive or autonomic components (table 2)
Dur: Variable, LOC±, PC±
Variable
UNKNOWN
Epileptic spasms
Sudden flexion, extension or mix of proximal truncal muscles, typically in series Dur: 1-2 s; LOC-, PC-
Gen’d high-amp slow wave then lowamp fast activity or attenuation
PC, postictal confusion; LOC, loss of consciousness; Dur, duration. Adapted from the ILAE Commission on Classification & Terminology, epilepsydx.org & Epilepsia 2010;51:676.
Adapted from Continuum. Epilepsy 2007;13(4):Chapter 1.
Typical Features of Focal Seizures by Region of Onset
Temporal lobe
Mesial TL: Aura (e.g., epigastric, psychic, affective, olfactory), impaired consciousness, fixed stare, early oroalimentary automatisms, limb automatisms (bilateral or ipsilateral to focus), dystonic posturing, postictal confusion, & amnesia
Lateral TL: Aura, e.g., hallucinations (auditory, complex perceptual or experiential); language dysfxn; late oroalimentary automatisms; late manifestations ≈ mesial TL
Frontal lobe
Brief, often in clusters; little or no postictal confusion; rapid generalization; motor si/sx (clonic, tonic, postural); hyperkinetic complex or bizarre automatisms; sexual automatisms; frequent falls; nocturnal predominance; SE
Occipital lobe
Elementary visual hallucinations, esp in contralateral hemifield; blindness; sensation of eye mvmt; eye deviation (contralateral or ipsilateral); forced blinking; variable spread to PL (sensory sx), TL/OL (formed visual hallucinations), mesial TL
Parietal lobe
Somatosensory auras; receptive aphasia (dom hem); neglect (nondominant hem); variable spread to OL (visual hallucination), mesial TL, precentral regions (motor)
Adapted from Continuum. Epilepsy 2007;13(4):Chapter 1.
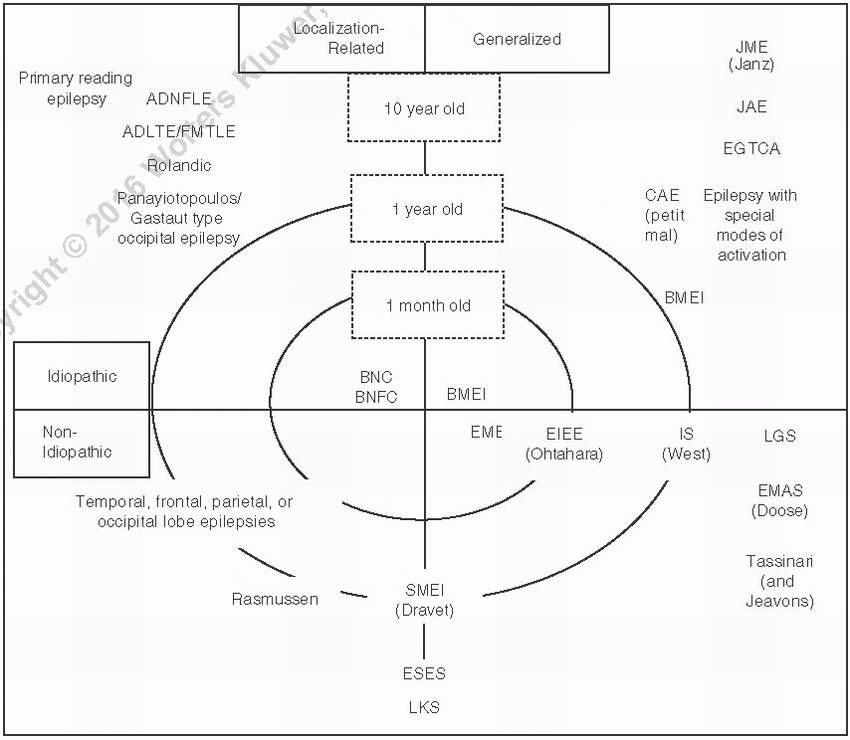
EPILEPSY SYNDROMES (PEDIATRIC EPILEPSY)
Epilepsy syndromes present in pediatric population, though many survive into adulthood.
Relevance: >50% epilepsy begins in childhood. Some sz types are unique to childhood (e.g., absence, myoclonic szs), may occur exclusively during specific neurodevelopmental stage (e.g., infantile spasms), & often have genetic underpinning.
Epilepsy syndromes are defined by: Age at onset, sz type, gender predominance, etiology [idiopathic/genetic, symptomatic, cryptogenic (cause suspected but not found), associated developmental delay, diurnal variability, precipitating factors (sleep deprivation, photic stimulation)], severity, family hx, developmental prognosis, & epilepsy outcome. Syndrome identification has implications for management, prognosis, research, genetics.
Only gold members can continue reading. Log In or Register to continue