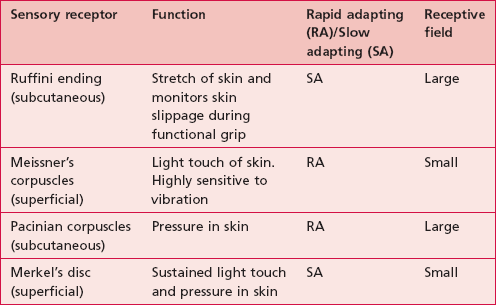
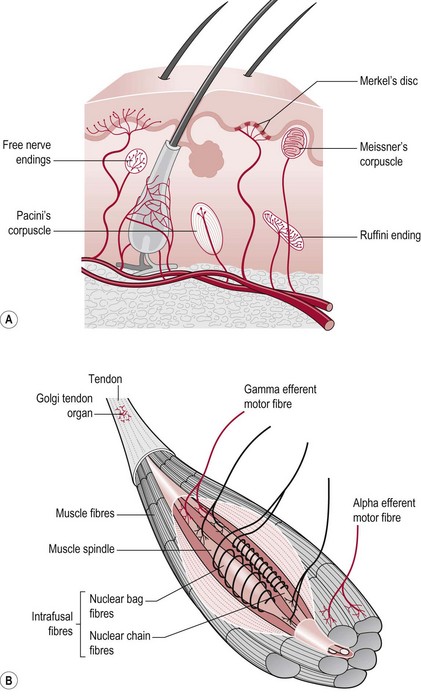
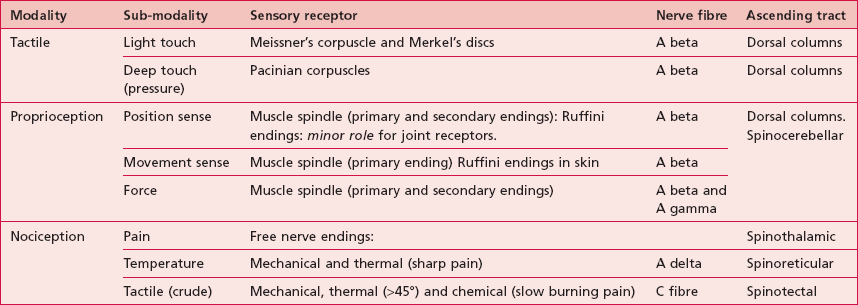
Chapter 23 The somatosensory system reacts to diverse stimuli from different sensory receptors, thermoreceptors (temperature), mechanoreceptors (physical distortion) and chemoreceptors (chemicals). Each sensory modality has a unique sensory receptor which is activated when a specific stimulus, within its receptive field, reaches a threshold intensity. This receptive field may be altered as a result of pathology when it can contribute to the experience of pain (S3.29) and abnormal sensation. The density of receptors is relevant to the ability to locate a stimulus (awareness) and to distinguish between two stimuli (discrimination). The duration of a sensory experience is related to a further characteristic of the sensory receptor termed ‘adaptation’. A rapidly adapting receptor responds to change and is therefore activated at the onset and termination of the stimulus only. A slowly adapting receptor responds continuously to a persistent stimulus. This should be borne in mind when assessing particular modalities. Figure 23.1 shows the main somatosensory receptors and Table 23.1 identifies the functional characteristics of these receptors. This afferent information from sensory receptors in the periphery is conducted along afferent neurons to the spinal cord (S2.13) and transmitted via the ascending tracts (S2.15) to the thalamus (S2.9), brain stem (S2.10) and higher centres (S2.7). Sensory input is systematically mapped on the contralateral primary somatosensory cortex (parietal lobe), then processed and integrated with other relevant information by the somatosensory association area (parietal lobe), basal ganglia (S2.11) and cerebellum (S2.12) before being acted upon. Functionally relevant information is often transmitted in the same anatomical ascending tract (S2.15) but in separate parallel pathways. For example, when holding an object, the information related to texture (light touch) and shape (proprioception) are both conveyed in the dorsal columns. This overlap in function may be important clinically as following a lesion, the adjacent preserved tracts may be able to assist in the lost function. Table 23.2 shows a summary of the functional anatomy related to the modalities described below. In terms of touch a hierarchy of sensory function was proposed by Fess (1990). The lowest level is the ability to identify a single stimulus (awareness). The hierarchy proceeds with the ability to distinguish between two stimuli (discrimination), the ability to differentiate different characteristics or strength of one stimulus (quantification) and the highest level is the ability to recognize objects by touch alone (recognition). This hierarchy suggests that if the higher levels are intact, the lower levels do not need to be assessed. The sensation of light touch allows us to be aware of tactile stimuli, including situations as innocuous as the clothes we wear, but also has a role in warning us of impending damage. Following a neurological lesion, a patient may become hypersensitive to touch, when even clothes may initiate a sensory experience and an inappropriate motor response. This altered sensation may also be perceived as pain, paraesthesia or dysaesthesia (S3.29). In a scenario where a patient becomes hyposensitive to light touch, the lack of awareness of limbs particularly, may result in soft tissue injury. Pain serves to notify the nervous system about tissue damage that has occurred. Although pain can be elicited without tissue damage (neurogenic pain) (S3.29), nociceptive pain will remain the focus here. The sensory receptors sensitive to nociceptive stimuli are free nerve endings, however not all noxious stimuli is perceived as pain because the response to a stimuli is highly subjective. The free nerve endings are much less specialized than other receptors and may respond to mechanical, thermal or chemical stimuli. Our sense of proprioception is complex and results from integration of information from several sources, visual (S2.10, S3.27), vestibular (S2.10) and somatosensory systems. In this text, proprioception is defined as consisting of three sub-modalities (Riemann and Lephart 2002a,b); the ability to sense: • Position sense (body parts and their relationship to each other) • Movement sense (sometimes referred to as kinaesthesia) Historically, joint receptors have been considered to have an important role in proprioception, however recent studies have shown that this is not the case in most joints (Proske and Gandevia 2009). In fact, the major sensory receptors involved in position and movement sense are muscle spindles and stretch receptors in the skin (Ruffini endings). The skin receptors have a greater role in circumstances where the controlling muscle is distant to the joint being moved (e.g. fingers) (Collins et al. 2005) and in the case of two joint muscles (Sturnieks et al. 2007). Ruffini endings have been found to be accurate within 2° in relation to change of joint angle in the fingers and deficits contribute to altered timing and force of grip in stroke (Blennerhassett et al. 2007). • Inability to interact with the environment • Inability to produce skilled movement (Campbell 2000) • Significant reduction in functional ability (Fang et al. 2003, Tyson et al. 2008) and quality of life (Forsaa et al. 2008) • Production of central neuropathic pain (S3.29) (Widerstrom-Noga et al. 2002).
Sensation
What is sensation?
Sensory receptors
Sensory pathway
 Clinical hints and tips
Clinical hints and tips
Sensory modalities
Tactile
Light touch
Nociception
Pain (S3.29)
Proprioception
Why do I need to assess sensation?
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Neupsy Key
Fastest Neupsy Insight Engine
 Clinical hints and tips
Clinical hints and tips




