Sensory Nerve Conduction Studies
QUESTIONS
1. For sensory conduction studies, the gain is usually set at:
A. 1 μV
B. 20 μV
C. 100 μV
D. 200 μV
View Answer
1. (B): The sensory responses are very small, and technical factors and electrical noise may distort the waveforms. For sensory conduction studies, the gain is usually set at 10 to 20 μV. The gain is set at microvolts; millivolts are used to measure motor conduction results. (Preston and Shapiro 1998, p. 27)
2. The following statements are correct except:
A. The recording electrodes are placed in line over the nerve with an interelectrode distance of 3 to 4 cm
B. Most sensory nerves require a current in the range of 5 to 30 mA to achieve supramaximal stimulation
C. Sensory nerves require a higher threshold for stimulation than do motor fibers
D. In sensory studies, a conduction velocity can be calculated using one stimulation site alone
View Answer
2. (C): The sensory nerves have a low threshold for stimulation compared to motor fibers and require a lower current (5 to 30 mA) to achieve supramaximal stimulation. The recording electrodes are placed in line over the nerve with recommended interelectrode distance of 3 to 4 cm. The active electrode is placed closest to the stimulator. Unlike motor studies, in sensory studies a conduction velocity can be calculated using one stimulation alone as the recording electrode is measuring a nerve action potential. (Preston and Shapiro 1998, p. 29)
3. Antidromic recording of sensory nerves is superior to orthodromic technique because:
A. Amplitude is higher using antidromic stimulation
B. The electrodes are closer to the nerve
C. It is less subject to noise or other artifact
D. The entire nerve is stimulated including the motor fibers
View Answer
3. (A): The antidromic technique results in stimulation of the entire mixed nerve including the motor fibers resulting in CMAP along with SNAP. This may become a problem when SNAP imbeds in CMAP. At times if SNAP is absent, one can misread CMAP as SNAP. The amplitude with antidromic technique is higher because the recording electrodes are closer to the nerve and is less subjected to noise or artifact. (Preston and Shapiro 1998, p. 32)
4. Myelinated fibers conduct at a velocity of approximately:
A. 100 m/s
B. 65 m/s
C. 30 m/s
D. 10 m/s
View Answer
4. (B): The myelinated fibers conduct at a velocity of approximately 65 m/s, while the unmyelinated fibers conduct at a velocity of 1 to 2 m/s. Most fibers lie between these two extremes. (Preston and Shapiro 1998, p. 37)
5. Demyelination is associated with:
A. Marked slowing of conduction velocity (slower than 85% of the lower limit of normal)
B. Marked prolongation of distal latency (longer than 110% of upper limit of normal)
C. Low compound motor action potential (CMAP) amplitude
D. Drop in amplitude in proximal stimulation compared to the distal stimulation
View Answer
5. (D): The drop in amplitude in proximal stimulation (conduction block) compared to the distal stimulation is seen with focal demyelinating neuropathies. Marked slowing of conduction velocity (slower than 75% of the lower limit of normal) is seen. Marked prolongation of distal latency (longer than 130% of upper limit of normal) is also a feature of demyelinating conditions. The CMAP amplitude can be normal or reduced in demyelinating neuropathies depending on the degree of distal demyelination or superimposed conduction block. (Preston and Shapiro 1998, p. 39)
6. Routine nerve conduction studies are normal in _____% of patients with clinical symptoms and signs of carpal tunnel syndrome.
A. 5%
B. 20%
C. 30%
D. 40%
View Answer
6. (B): In patients with typical carpal tunnel syndrome (CTS), the median distal motor and sensory latencies, and minimum F-wave latencies are moderately to markedly prolonged. However, there is a group of patients with clinical symptoms and signs of carpal tunnel syndrome in whom these routine studies are normal (10% to 25%). In such patients, the electrodiagnosis of CTS may be missed. (Preston and Shapiro 1998, p. 238)
7. Carpal tunnel syndrome electrodiagnostic studies usually show (see Fig. 13.1):
A. Higher amplitude of median CMAP compared to ulnar nerve
B. The median nerve orthodromic absolute onset sensory latency is delayed by >3.7 ms
C. The median nerve orthodromic sensory latency is delayed by >2.0 ms compared to the ulnar nerve sensory distal latency
D. The median nerve orthodromic sensory latency is delayed by >0.2 ms compared to the ulnar nerve sensory distal latency
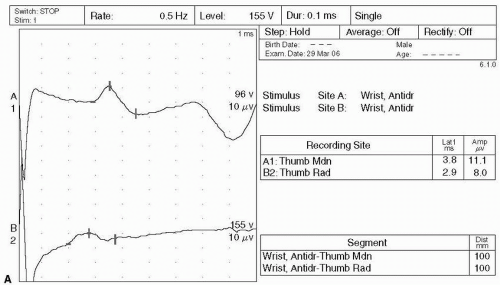 Figure 13.1. (A) Median versus radial sensory nerve conduction (SNC) and (B) median versus ulnar motor nerve conduction (MNC) |
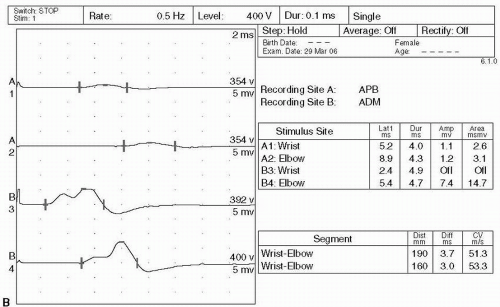 Figure 13.1. (Continued) |
View Answer
7. (D): A CTS study should show the median nerve orthodromic sensory latency delayed by >0.2 ms compared to the ulnar nerve. The median CMAP amplitude is usually much higher than ulnar. The picture depicts an orthodromic sensory response. The median nerve orthodromic sensory absolute latency >3 ms is usually abnormal, however, the absolute latency can be delayed because of multiple factors and therefore, absolute latency delay is usually not taken as a marker of CTS. (Preston and Shapiro 1998, p. 238)
8. Median- versus ulnar-comparison tests are good tests to confirm carpal tunnel syndrome for the following reasons except:
A. They create an ideal internal control
B. Distance is different
C. Temperature is constant
D. Nerve fiber size is constant
View Answer
8. (D): In comparison studies, identical distances are used between the stimulator and recording electrodes for median and ulnar nerves. These techniques create an ideal internal control in which several variables that are known to affect conduction time are held constant, for example, distance, temperature, age, and nerve size. If the distal motor and sensory latencies are normal then comparison studies often are very helpful because they rely on patient’s own nerve rather than on population normal values. (Preston and Shapiro 1998, p. 238)
9. Median- versus ulnar-sensory nerve short latency midpalmar study comparison test is abnormal if the median latency is delayed by more than _____ the ulnar latency.
A. 0.1 ms
B. 0.2 ms
C. 0.3 ms
D. 0.4 ms
View Answer
9. (D): In comparison studies, very small difference (0.4 ms) between median and ulnar nerve is considered abnormal. Attention must be paid to all technical factors to avoid false-positive results. Technical factors such as distance measurement, stimulus artifact, supramaximal stimulation, and electrode placement can all affect the results. It is essential to avoid over stimulation because it can cause unintentional stimulus spread to an adjacent nerve. (Preston and Shapiro 1998, p. 238)
10. In a patient with right foot pain, a sural and plantar sensory response is unmeasurable. The lesion can be present in the following except:
A. Tarsal tunnel syndrome
B. Sciatic lesion
C. Lumbosacral plexus lesion
D. Peripheral neuropathy
View Answer
10. (A): The absence of a sural sensory response is not seen in tarsal tunnel syndrome. Tarsal tunnel syndrome is the compression of distal tibial nerve under the flexor retinaculum on the medial side of ankle. This results in a delayed or absent response in the medial and lateral plantar nerve responses. The absence of sural sensory response indicates a lesion above the tarsal tunnel syndrome and can be affected by a sciatic nerve lesion, lumbosacral plexopathy, and peripheral neuropathy. (Preston and Shapiro 1998, p. 331)
11. All of the following statements are correct except:
A. Orthodromic stimulation of the plantar sensory nerve produce a small amplitude response
B. Bilateral absent plantar sensory responses in middle aged or older individuals have no significance
C. In suspected tarsal tunnel syndrome, one side abnormal plantar response is diagnostic of tarsal tunnel syndrome
D. Medial and lateral plantar sensory potentials are unobtainable even in healthy subjects
View Answer
11. (A): Evaluation of tarsal tunnel syndrome is greatly simplified if one side is abnormal as the other side acts as a control (Fig. 13.3). Surface plantar sensory studies are difficult to perform in healthy subjects. Orthodromic stimulation of the plantar sensory nerve produces very small amplitude responses, making it necessary to average many potentials. Medial and lateral plantar sensory potentials are unobtainable even in healthy subjects and similarly bilateral absent plantar sensory responses in middle-aged or older individuals have no significance. (Preston and Shapiro 1998, p. 331)
12. Small fiber peripheral neuropathy is seen in all of the following conditions except:
A. Diabetes
B. Fabry disease
C. Diphtheria
D. Tangier disease
View Answer
12. (C): Only a few peripheral neuropathies preferentially affect small fibers. Diabetes, Fabry disease, and Tangier disease all cause small fiber peripheral neuropathy while diphtheria does not typically affect the small fibers. Small fiber neuropathy manifests as an autonomic dysfunction and a distal peripheral sensory deficit for pinprick and cold, often associated with painful paresthesia. Routine nerve conduction studies assess only large myelinated fibers and can be completely normal in small fiber neuropathies. (Preston and Shapiro 1998, p. 356)
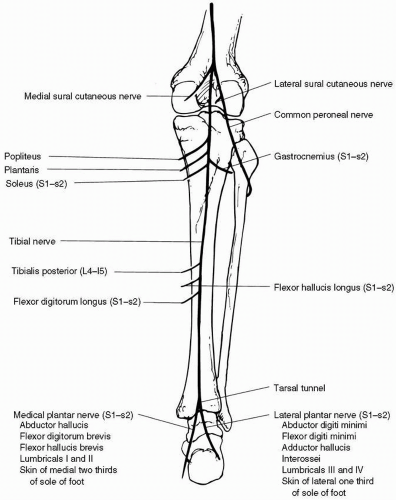 Figure 13.3. The tibial nerve (From Brazis PW, Masdeu JC, Biller J. Localization in clinical neurology, 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2007)
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|


