♦ Preoperative
Operative Planning
- Repair of skull defect can be performed acutely in clean cases
- In cases of hemicraniectomy for control of elevated intracranial pressure, repair is performed following resolution of intracranial hypertension
- In contaminated cases, wait 3 to 6 months before repair is attempted
- Shunt may be placed preoperatively in those with external hydrocephalus
Equipment
- Major craniotomy tray
- Mayfield head holder
- High-speed drill
- Methyl methacrylate, hydroxyapetite cement, or substitute (Norian [Norian Corporation, Cupertino, CA], Bonesource [Stryker-Leibinger, Kalamazoo, MI], HydroSet [Stryker], etc.) (optional)
- Titanium microplates and screws (optional)
- Titanium mesh (optional)
Operating Room Set-up
- Headlight
- Loupes
- Bovie cautery and bipolar cautery
Anesthetic Issues
- Intravenous antibiotics (cefazolin 2 g) should be given 30 minutes prior to incision
♦ Intraoperative
Positioning
- Depends on location of defect
- Consider placing lumbar drain to remove cerebrospinal fluid, thus decreasing intracranial pressure and allowing more room for cranioplasty
Planning of Sterile Scrub and Prep
- As for craniotomy
Exposure
- Typically, previous incision is used and/or previous laceration is in part used
- Flap is carefully elevated from underlying scar and dura; use of blunt dissection and/or sharp dissection
- Brain may be adherent to scar and skin in cases of incompetent dura
- Edges of bone identified with a curette or periosteal elevator
- Dura covered with compressed Gelfoam or DuraGen
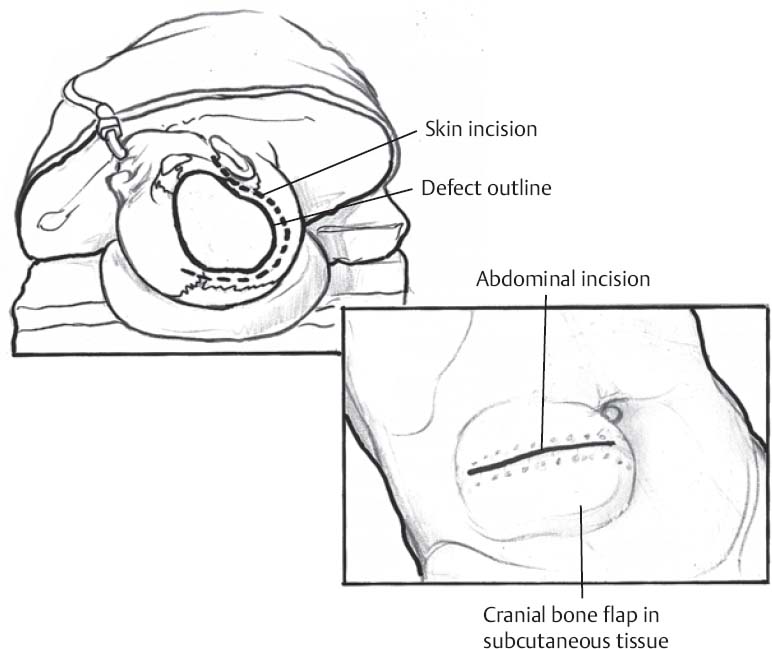
Fig. 86.1 Bone flap removed during prior decompressive hemicraniectomy may be retrieved from subcutaneous storage in abdomen.
Only gold members can continue reading. Log In or Register to continue
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


