Sleep and Circadian Rhythms
NORMAL SLEEP
Sleep remains a mystery. We spend roughly a third of our lives in this suspended state. All mammals sleep, as does most of the animal kingdom. Even the fruit fly sleeps—although not enough. Most people look forward to sleeping, especially if they have been deprived of sleep. Without enough sleep, people function as poorly as if they are drunk. Significant sleep deprivation will cause psychosis and physical problems. What is it that happens to us when we sleep?
The average length of sleep is approximately 7.5-hours per night (Figure 15.1). Remarkably, some people, called nonsomniacs, require much less. Meddis studied a retired nurse who was happily functioning on an hour of sleep a night. She reported she had needed little sleep all her life. When studied in Meddis’s sleep laboratory, she did not sleep the first night and then slept, on average, only 67 minutes for each of the remaining four nights. She did not complain of being tired or wanting more sleep. (As an aside, some in the psychiatric community might diagnose this woman with a bipolar spectrum disorder, although her condition may simply be a variant of sleep need.)
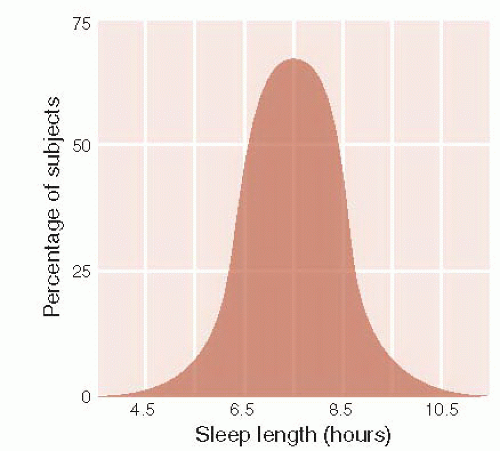 FIGURE 15.1 • The duration of sleep for adults is normally distributed around a mean of 7.5-hours per night. (Adapted from Hobson JA. Sleep. New York, NY: Scientific American Library; 1989.) |
Most people show deterioration in performance when deprived of sleep. Figure 15.2 shows the results of neurobehavioral tasks for subjects deprived of differing amounts of sleep. One group was totally sleep deprived for 3 days, two other groups were restricted to 6 or 4-hours of sleep per night for 14 days, and the control group got 8-hours of sleep per night. Figure 15.2A shows the effects of sleep restriction on a sustained attention task, whereas Figure 15.2B shows the effects on a test of memory. Note how chronic sleep deprivation takes a toll on the subjects’ performance as the study progresses. Of interest, the subjects were largely unaware of their impairments—a finding that is not uncommon when cognition declines.
A recent intervention with medical interns working in an intensive care unit in a Boston hospital demonstrated a practical application of this knowledge. Interns who had their workday limited to 16-hours (compared with the traditional 24+ hours) got more sleep each week and made half the attentional errors during on-call nights compared with the interns following the traditional schedule.
Stages of Sleep
For centuries, sleep had been considered a passive, uniform process that simply restored the body. That changed in 1953 when Nathaniel Kleitman and Eugene Aserinksy examined electroencephalographic (EEG) recordings from sleeping healthy subjects. They discovered that sleep comprises
different stages that repeat in characteristic patterns throughout the night. They identified the three states of consciousness as awake, non-rapid eye movement (non-REM) sleep, and rapid eye movement (REM) sleep. Non-REM sleep has been further subdivided into four stages.
different stages that repeat in characteristic patterns throughout the night. They identified the three states of consciousness as awake, non-rapid eye movement (non-REM) sleep, and rapid eye movement (REM) sleep. Non-REM sleep has been further subdivided into four stages.
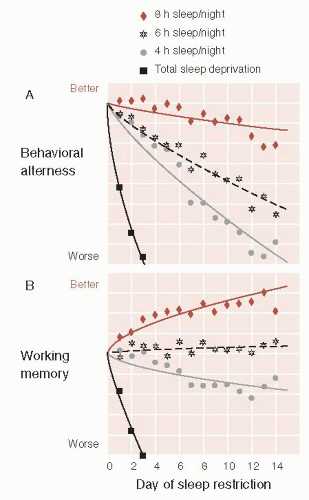 FIGURE 15.2 • The effects of total sleep deprivation for 3 days and chronic sleep restriction for 14 days are measured with neurobehavioral tasks. The Psychomotor Vigilance Task (A) measures alertness and attention. The Digit Symbol Substitution Task (B) measures working memory. (Adapted from Van Dongen HP, Maislin G, Mullington JM, et al. The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep. 2003;26(2):117-126.) |
Electroencephalographic Patterns
Figure 15.3 shows the characteristic EEG patterns during the different stages of sleep. From an awake state to the deepest sleep of stage 4, there is a progression of decreasing frequency and increasing amplitude of the EEG activity. Stage 1 sleep, also called the drowsy period, is so light that most people when awoken from this stage will say that they were not asleep. Stage 2 sleep shows the development of sleep spindles, which are periodic bursts of activity resulting from interactions between the thalamus and the cortex. Stage 3 and 4 sleep, also called slow wave sleep (SWS), are the deepest stages of sleep characterized by the development of delta waves. REM sleep is the most unusual finding that Kleitman and Aserinksy discovered. In REM sleep, the EEG activity is remarkably similar to the awake state, but the body, or at least major muscles, is paralyzed.
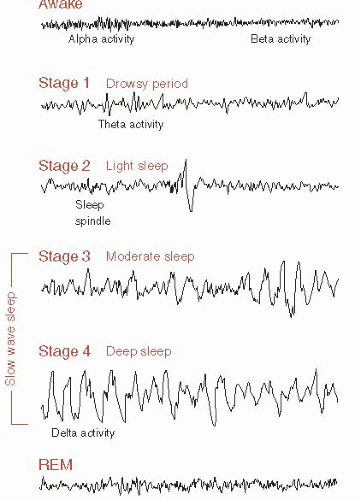 FIGURE 15.3 • Characteristic electroencephalographic rhythms during the stages of consciousness. REM, rapid eye movement. (Adapted from Horne JA. Why We Sleep: The Functions of Sleep in Humans and Other Mammals. Oxford: Oxford University Press; 1988.) |
In a typical night, a person cycles through five episodes of non-REM/REM activity (Figure 15.4A). The first REM episode occurs after approximately 90 minutes of sleep. The time to the first REM occurrence is called REM latency and is usually reduced in patients who are exhausted as well as those with depression, narcolepsy, and sleep apnea. The deepest stage of sleep occurs only in the early phases of the night. The REM episodes increase in length as the night unfolds.
POINT OF INTEREST
All mammals sleep. Mammals living in the water are able to sleep, but still they must regularly surface for air. Additionally, from the day they are born until they die, dolphins are continuously moving and avoiding obstacles. They do not have a period of immobility that in terrestrial mammals marks the state of sleep. How do they do all this and still sleep?
Studies of EEG tracings of the bottlenose dolphin show that they rest one hemisphere at a time (see figure). Note how the large amplitude waves of SWS are only present in one hemisphere at a time. The eye contralateral to the brain hemisphere showing slow waves is usually closed while the other eye is almost always open. Lastly, these dolphins do not display REM activity, which may be an adaptation so they can keep moving.
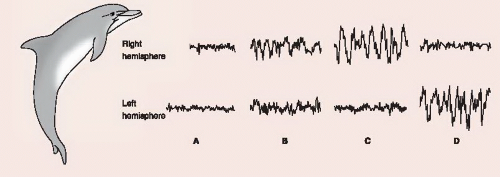 Electroencephalographic tracings from bottlenose dolphins. (Adapted from Mujhametov LM. Sleep in marine mammals. In: Borbely AA, Valatx JL, ed. Sleep Mechanisms. Munich: Springer; 1984 and Purves D, Augustine GJ, Fitzpatrick D, et al. Neuroscience. 3rd ed. Sunderland, MA: Sinauer; 2004.) |
Figure 15.4B shows some of the other physiologic changes that take place during the stages of sleep. The most remarkable findings are the differences in physiologic activity between non-REM and REM sleep. Non-REM sleep is characterized by limited eye movement and a decrease in muscle tone, heart rate, and respirations. Metabolic rate and body temperature are also decreased in these stages. They reach their lowest levels during stage 4 sleep. REM sleep, as the name implies, is characterized by rapid, darting movements of the eyes along with paralysis of most major muscle groups. Heart rate and respirations increase almost to the level found when awake. Penile/clitoral erections also occur during REM sleep—a finding that helps rule out physiologic impotence.
Muscle Tone
Muscle activity varies depending on the phase of sleep. During non-REM sleep, the muscles are capable of movement, but they rarely do so. On the other hand, REM sleep is characterized by a loss of skeletal muscle tone. Respiratory muscles along with the muscles of the eyes and the tiny muscles of the ear remain active in REM sleep.
Brain Imaging
Brain imaging studies during sleep reveal a pattern that is consistent with EEG findings. During non-REM sleep, positron emission tomography (PET) studies show decreased cerebral blood flow and energy metabolism. The greatest decreases correlate with greater depth of sleep. Alternatively, REM sleep shows a cerebral energy metabolism, which is equal to that occurring during awakening.
William Dement, a prominent sleep researcher from Stanford, has eloquently summarized the difference between the phases of sleep. He has characterized non-REM sleep as an idling brain in a movable body. In contrast, REM sleep is an active, hallucinating brain in a paralyzed body.
Changes with Aging
Total sleep duration and the proportions of time spent in various stages change as people age. Figure 15.5 shows the duration of sleep across the life span. Neonates (on the left of the figure) spend most of their time sleeping, with a large percentage of that time in REM sleep. Some have suggested that REM serves a developmental purpose and this is why neonates and young children require so much time in this phase.
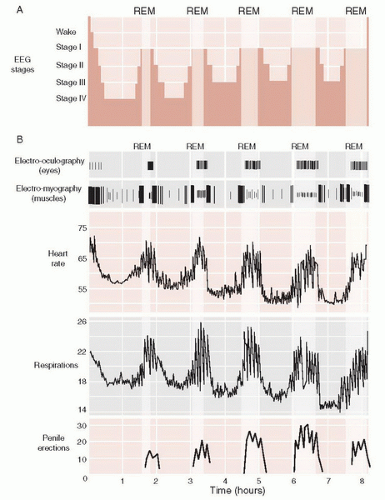 FIGURE 15.4 • Physiologic changes in a healthy volunteer during 8 hours of sleep. REM, rapid eye movement. (Adapted from Purves D, Augustine GJ, Fitzpatrick D, et al. Neuroscience. 5th ed. Sunderland, MA: Sinauer; 2011.) |
DISORDERS
SLEEPWALKING AND NIGHT TERRORS
Approximately 40% of people are sleepwalkers as children, although few are sleepwalkers as adults. This behavior usually occurs in the first stage 4 non-REM period of the night. In a typical episode, the child’s eyes will be open and the child will avoid obstacles when moving about the room or house. The cognition is clouded and the child will usually have no memory of the event. The best intervention is to gently guide the sleepwalker back to bed.
Night terrors are characterized by extreme terror and an inability to be awakened. Typically occurring in children between the ages of 4 and 7, this condition affects only approximately 3% of the population. As with sleep walking, it develops in the deep stages of non-REM sleep. Night terrors are not to be confused with nightmares, which are vivid dreams during REM sleep.
The child appears in a state of panic, and may even scream and cry. Fortunately, it usually returns to sleep in 10 to 20 minutes and little is remembered the next day. The greatest toll may be on the parents who have to comfort the frightened child. The best intervention is support.
On the right side of Figure 15.5 is a meta-analysis of sleep duration from childhood to old age. Note the gradual reduction in the deepest stages of sleep and the increase in awakening after sleep onset as people age. Dissatisfaction with sleep is a common complaint in the elderly, and the origins of those complaints can be seen in this figure.
Dreaming
Historically, it has been believed that dreaming is limited to REM sleep. A thorough analysis of what people are experiencing at different stages of consciousness reveals that dreams occur in all stages of sleep, but the content varies. Researchers gave college students a pager and instructed them to
sleep with a special nightcap that recorded eye and head movement (see Figure 15.6A). The students were considered to be in non-REM sleep when there was an absence of eye movement. REM sleep was defined as rapid eye movements without head movement. The students dictated what they were doing, thinking, and feeling when they were paged or spontaneously awoke.
sleep with a special nightcap that recorded eye and head movement (see Figure 15.6A). The students were considered to be in non-REM sleep when there was an absence of eye movement. REM sleep was defined as rapid eye movements without head movement. The students dictated what they were doing, thinking, and feeling when they were paged or spontaneously awoke.
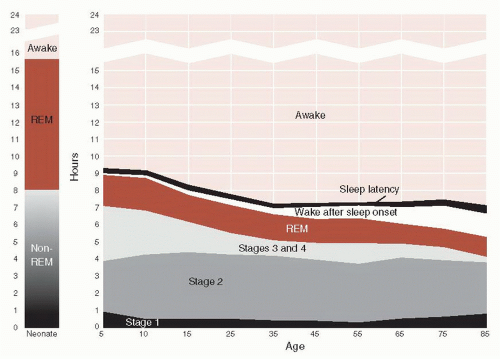 FIGURE 15.5 • Sleep duration across the life span. Neonates are shown on the left and on the right is a meta-analysis of sleep parameters in healthy individuals across the life span. REM, rapid eye movement. (Adapted from Ohayon MM, Carskadon MA, Guilleminault C, et al. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: developing normative sleep values across the human lifespan. Sleep. 2004;27(7):1255-1273.) |
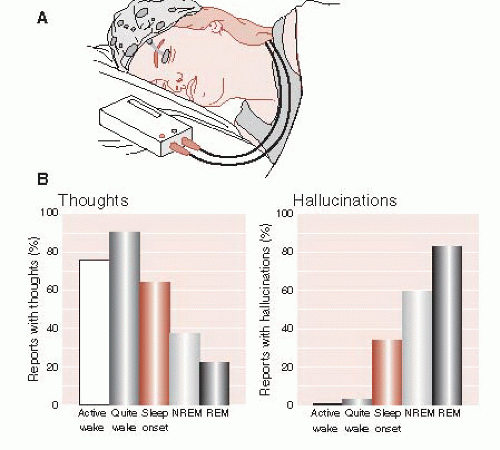 FIGURE 15.6 • A special home-based sleep-monitoring system (A) allows researchers to correlate dream content with the stage of consciousness (B). REM, rapid eye movement. (Adapted from Fosse R, Stickgold R, Hobson JA. Brain-mind states: reciprocal variation in thoughts and hallucinations. Psychol Sci. 2001;12(1):30-36.) |
The results showed that the subjects had dreams at all stages of sleep; however, the nature of dreams was different. In non-REM sleep, the dreams are more thoughts—as though the person is solving a problem. In REM sleep, the dreams are illogical, bizarre, and even hallucinatory. Figure 15.6B shows the decrease in thoughts as the subject goes from an awake state to REM sleep and the corresponding marked increase in hallucinations.
NEURONAL CIRCUITS
Until the 1940s, sleep was generally conceptualized as the body’s reaction to the lack of stimulation, that is, the brain passively turns “off” when there is no input. We now know that sleep is an active process initiated and terminated by different regions of the brain.
Suprachiasmatic Nucleus
The master clock of the brain is the suprachiasmatic nucleus (SCN) located in the anterior hypothalamus (Figure 15.7). The SCN orchestrates circadian rhythms throughout the brain and body. The SCN is synchronized (entrained) by signals from the retina, which are activated by inputs from the sun. When humans are prevented from receiving cues about the solar day (such as living in a cave for weeks), the 24-hour sleep-wake cycle will gradually increase to approximately 26-hours—a condition that is called free-running.
The SCN is made up of some of the smallest neurons in the brain and has a volume that is approximately 0.3 mm3. Output from the SCN synchronizes other cellular oscillators throughout the brain and body. Studies with hamsters have established the
crucial role this tiny collection of neurons play in the regulation of sleep-wake cycles. Figure 15.8A shows how recordings of the time a hamster spends on the running wheel can be used to establish their circadian rhythm. When the SCN is ablated, the 24-hour rhythm is lost and no regular pattern can be identified. If the hamster receives a transplant from a strain of mutant hamsters with a 22-hour circadian rhythm, the foreign rhythm becomes established.
crucial role this tiny collection of neurons play in the regulation of sleep-wake cycles. Figure 15.8A shows how recordings of the time a hamster spends on the running wheel can be used to establish their circadian rhythm. When the SCN is ablated, the 24-hour rhythm is lost and no regular pattern can be identified. If the hamster receives a transplant from a strain of mutant hamsters with a 22-hour circadian rhythm, the foreign rhythm becomes established.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


