Therefore, one can expect the mandatory increase in PaCO2 and reduction in PaO2 of 2 to 8 mm Hg and 3 to 10 mm Hg, respectively. Regardless of the change in PaO2, the SaO2 declines only by <2% in this scenario, given the characteristics of the oxyhemoglobin dissociation relationship (2). In individuals with normal pulmonary function and at sea level, there is relatively little consequence to SaO2. The impact of sleep in patients with COPD has been long-studied and, indeed, poses several challenging management considerations. Chronic bronchitis patients—the “blue bloaters”—are more likely to be hypoxemic and hypercapnic as compared to patients with advanced emphysema, the so-called “pink puffers” (3). Patients with COPD have been noted to demonstrate significant increase in mean pulmonary artery pressures and PaCO2 levels when going from wakefulness to sleep (4). The tendency for worsening nocturnal hypoxemia in these patients, coupled with the pulmonary vasculature’s response of hypoxic vasoconstriction, predisposes to the development of pulmonary hypertension and cor pulmonale (5). These consequences may be partly explained by the effects of the potent pulmonary vasoconstrictor endothelin (ET)-1. Patients with COPD who desaturate at night have higher circulating levels of ET-1 in their sera than do those who do not desaturate (6).
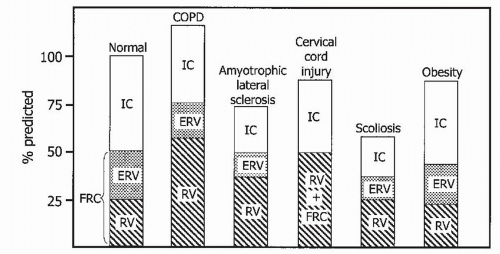 FIGURE 34-1 Lung volumes for a normal individual (far left) are compared with inflated lung volumes in a patient with COPD and reduced volumes in patients with various disorders of the thorax. IC, inspiratory capacity; ERV, expiratory reserve volume. (From Bergofsky EH. Respiratory insufficiency in mechanical and neuromuscular disorders of the thorax. In: Fishman AP, ed. Pulmonary diseases and disorders. New York: McGraw-Hill, 1980:1563, with permission.) |
Patients who desaturate during exercise
Nonobese patients with moderate to severe COPD with progressive decline in arterial blood gases (ABGs)
Hypercapnic patients with severe chronic bronchitis
Pulmonary and systemic hypertension
Congestive heart failure (CHF)
having allergies; no particular asthma drug was associated with a lessening of symptoms (11). Serial measurements of peak expiratory airflow have shown that airflow obstruction in asthmatic patients peaks between 3:00 and 4:00 AM (12). As described in the next section, this is part of the reason why asthmatic patients are more likely to present to the emergency department between midnight and 8:00 AM, 40% of their calls to physicians occur between 11:00 PM and 7:00 AM, and 42% to 53% of fatal asthma exacerbations occur at night (12-15).
TABLE 34-1 A CLINICAL CLASSIFICATION OF ILDS (PARTIAL LIST) | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Airway inflammation
Circadian rhythm changes in parasympathetic tone and hormone levels
Allergens and airway cooling
Gastroesophageal reflux
Mucociliary clearance
Bronchial hyperactivity
More specific genetic testing for mutations of the CFTR gene can be obtained if results and clinical information are equivocal (16).
have also found significant differences in the saturation data obtained online real time (high sampling rates) and those values obtained from memory (low sampling rates) in unattended studies. Desaturation indexes obtained from memory have been found to be significantly lower than those obtained online (40). Studies have confirmed lower sensitivities and higher specificities using longer averaging times settings (e.g., 12 seconds) and memory display mode (40). Faster recording settings (shorter averaging times) and online display mode give rise to higher sensitivity and lower specificity. Therefore, the default settings must be known to the user and the interpreter. Faster recording settings and online display are the methodology of choice.
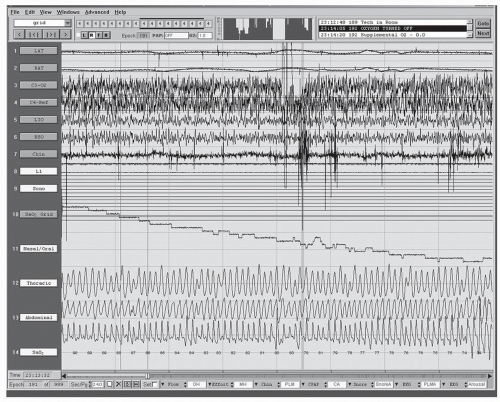 FIGURE 34-2 Periods of alveolar hypoventilation (gradual decline In Sao2 channel 10) during sleep (30-second epoch) may go undetected as the nasal/oral flow (thermistor) and chest and abdominal effort (piezoelectric belts) signals remain essentially unchanged. Channels 1 and 2, left and right anterior tibialis electromyogram; channels 3 and 4, left and right central electroencephalogram; channels 5 and 6, left and right occipital electroencephalogram; channel 7, chin electromyogram; channels 8 and 9, not used; channel 10, oxygen saturation; channel 11, nasal and oral flow sensors; channels 12 and 13, thoracic and abdominal effort sensors; channel 14, numeric oxygen saturation. |
severity of nocturnal desaturation in patients with COPD cannot be predicted with certainty. Hence, we can see the potential utility of overnight oximetry. The causes of the nocturnal desaturation include hypoventilation, coexisting sleep apnea, reduction in FRC, and altered ventilation-perfusion matching, as previously mentioned. The benefit of nocturnal oxygen therapy in patients with a daytime PO2 of >60 mm Hg, but nocturnal desaturation, is unproved. However, many clinicians will prescribe oxygen treatment if there is prolonged desaturation or evidence of end-organ dysfunction (cor pulmonale).
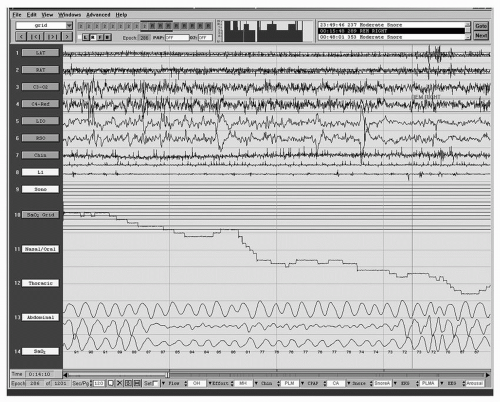 FIGURE 34-3 Periods of alveolar hypoventilation during sleep undetected by flow (thermistor) but demonstrated on the chest and abdominal effort channels (piezoelectric belts). Channels 1 and 2, left and right anterior tibialis electromyogram; channels 3 and 4, left and right central electroencephalogram; channels 5 and 6, left and right occipital electroencephalogram; channel 7, chin electromyogram; channels 8 and 9, not used; channel 10, oxygen saturation; channel 11, nasal and oral flow sensors; channels 12 and 13, thoracic and abdominal effort sensors; channel 14, numeric oxygen saturation. |
patients with severe CF had reduced sleep efficiency (71%) and frequent awakenings, as well as lower mean SaO2, when compared with 10 healthy controls. Furthermore, patients with CF were sleepier, with reduced sleep latency on multiple sleep latency test (MSLT) (6.7 minutes). These findings correlated with more reported fatigue and lower levels of happiness and activation as well as impaired cognitive function. Sleep-related complaints such as sleep-onset difficulties, sleep-maintenance trouble, and snoring are commonly seen in adults and children with CF. Children and adolescents with CF have decreased sleep efficiency, prolonged REM latency, and decreased REM sleep percentage when compared with controls (44). Children with stable CF have more frequent nocturnal cough than do children without CF. The cough is more severe with advancing disease and occurs most frequently in the first hour of sleep (45).
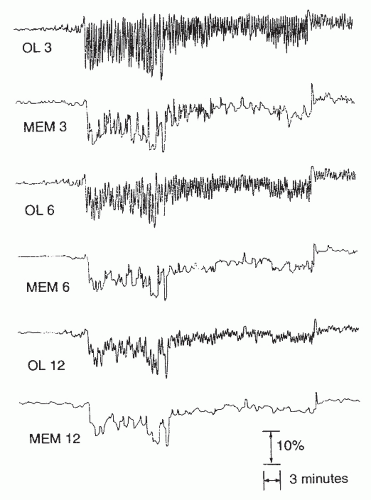 FIGURE 34-4 Cyclic desaturations in a patient with OSA depicted by oximetry. The oximetry data were recorded either online (OL) or from the oximeter’s memory function (MEM) at three different recording settings (3,6, and 12 seconds), which equate to averaging time and response time. (From Davila DG, Richards KC, Marshal BL, et al. Oximeter performance: the influence of acquisition parameters. Chest 2002;122:1654, with permission.) |
Dolly and Block (53) performed a randomized, placebocontrolled study on the effects of medroxyprogesterone acetate at 20 mg t.i.d. in patients with COPD and SDB. Four weeks of therapy was associated with increased awake mean PaO2 and reduced PaCO2 but no change in number of apneas, hypopneas, desaturation events, or lowest SpO2.
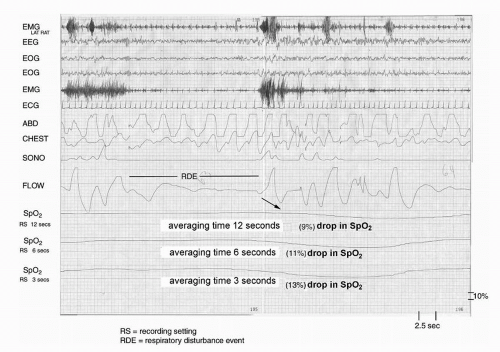 FIGURE 34-5 A RDE with pulse oximetry monitoring at three different recording settings (RS) at averaging times of 3, 6, and 12 seconds. Channels: EMG, electromyogram; EEG, electroencephalogram; EOG, electrooculogram; ECG, electrocardiogram; ABD (abdominal) and chest effort (piezoelectric belts); SONA, sonogram; flow, thermistor sensors; SpO2, oxygen saturation. |
patients with COPD admitted to the intensive care unit for acute exacerbation. The standard treatment group was treated with up to 5 L/min supplemental oxygen to maintain the SpO2 at >90%, in addition to bronchodilators, antibiotics, and steroids. The group treated with NIV received similar therapy. The individuals treated with NIV experienced reduced morbidity, mortality, and length of hospital stay.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


