By the year 2050, it is predicted that approximately one fifth of the population will be over 65 years of age. In 1900, only 4% of the population was over 65. This increase will have profound medical, economic, and psychosocial consequences. Because sleep complaints increase with age, the medical community needs to educate itself on changes in sleep with age. This chapter describes those changes as well as the most common diagnoses and treatments of sleep disorders seen in the elderly patient with neurodegenerative disease.
Although the normal sleep architecture changes with age, with less time spent in the deeper levels of sleep, sleep disturbances in the older population are often multifactorial. The sleep disturbance may be due to a primary sleep disorder, such as obstructive sleep apnea (OSA), periodic limb movements of sleep (PLMS), or restless leg syndrome (RLS), or it may be secondary to circadian rhythm changes, medical problems, psychiatric conditions, polypharmacy, or psychosocial factors. Conversely, when sleep disorders become chronic, they may exacerbate medical and psychiatric illnesses. Chronic sleep disorders or associated excessive daytime sleepiness (EDS) may result in disturbed intellect, impaired cognition, confusion, psychomotor retardation, or increased risk of injury, any of which can alter an individual’s quality of life or create social and economic burdens for caregivers.
SLEEP TESTS
Sleep is evaluated by recording electrical potentials from the brain [electroencephalography (EEG)], eye movements [electro-oculography (EOG)], muscle activity [electromyography (EMG)], heart rhythm [electrocardiogram (EKG)], body position (supine, left, right), oximetry, and respiratory activity (airflow, thoracic and abdominal excursion). Traditionally, sleep is generally recorded in the laboratory setting for one full night. This full night sleep recording is called a polysomnograph (PSG). It is a method of continuous and simultaneous recording of physiologic variables during sleep (249). It is indicated for the evaluation of patients suspected of having a sleep-related breathing disorder, unusual nocturnal spells, or unusual movements. A second recording, the Multiple Sleep Latency Test (MSLT) may be useful in quantitating the degree of sleepiness. This test measures an individual’s ability to fall asleep when given four or five nap opportunities throughout an average day. The MSLT is done during the day, following a nocturnal polysomnogram (249).
When patients are first recorded in the sleep laboratory, their anxiety about sleeping in a new and unfamiliar environment may lead to a recording that is not representative of their usual sleep. This is called the first night effect (3). Recently, technical advances allow for these types of recordings to be done in the home. Patients are set up with instrumentation in the laboratory, sent home, and asked to come back the following day after spending the night in their own bed. These home recordings or unattended monitoring reduce the first night effect, reduce costs, increase comfort, and reduce the waiting time for a study in some cases.
SLEEP STAGING
Sleep is divided into two states: nonrapid eye movement (NREM) sleep and REM sleep. NREM and REM sleep alternate throughout the night in a cyclical pattern. NREM sleep is further subdivided into stages 1, 2, 3, and 4. NREM sleep progresses from stage 1 (light sleep) to slow-wave sleep (SWS) (stages 3 and 4). With this progression from stage 1 to 4, there is a relative increase in the depth of sleep and the threshold for spontaneous arousals. Stage 1 sleep is a transition between wakefulness and sleep. Its characteristics include low-voltage, mixed-frequency EEG and slow rolling eye movements. The signatures of stage 2 sleep include sleep spindles and K-complexes. SWS refers to stages 3 and 4 sleep. It is characterized by high-amplitude (75 µV), slow-frequency (delta) waves (62). REM sleep is very distinct from light and SWS and is characterized by increased sympathetic activity, rapid eye movements, dreaming, and an increase in the depth and rate of breathing. REM sleep is accompanied by a low-voltage, mixed-frequency EEG and reduction of the EMG tone (muscle atonia). This is when the most elaborate dreams emerge. A physiologic sleep paralysis manifested by low EMG tone on the polysomnogram protects the patient from acting out dreams.
AGE-RELATED CHANGES IN SLEEP
With aging, the amount of time spent in SWS decreases; thus, the time spent in lighter levels of sleep increases. The proportion of REM sleep is generally preserved. However, the latency to the first REM period decreases, and the overall amount of REM sleep may decrease as a result of an overall reduction in nocturnal sleep time. Older adults also take longer to initiate sleep. They have a reduced total sleep time, frequent awakenings, and early morning awakenings and are more likely to have diurnal naps (83,167).
The prevalence of napping in older adults ranges from 25% to 80% (200,263). Studies that have used the MSLT to evaluate sleepiness in older persons have shown that, given the opportunity, they tend to fall asleep during the day faster than younger patients (61). This daytime sleepiness suggests that the older adults are not getting sufficient sleep at night. This is interpreted to mean that the need for sleep in older adults is not reduced, but rather that the ability to sleep is changed (10).
Studies that have looked at gender differences in the sleep of healthy elderly have found that women sleep better than men (38) and maintain sleep better than men (203). Recent studies evaluating the effects of menopause on sleep have found associated subjective complaints of insomnia. Objectively, menopause was found to prolong sleep latency, reduce REM sleep, and reduce total sleep time. Treatment with estrogen replacement therapy may alleviate these problems (268).
CLINICAL HISTORY
The clinical evaluation of an elderly patient with a sleep complaint involves a multidisciplinary approach. First, the clinical approach begins with a careful history taking of the present and past sleep history, as well as a detailed history of specific sleep complaints. Family history is always important as well as social history, in particular regarding alcohol and caffeine intake. Questions regarding polypharmacy and particular use of psychiatric medications may be a key in the initial evaluation.
Important questions that need to be asked when obtaining the sleep history are as follows. This information is supplemented by having the patient keep a careful sleep diary for several weeks.
Do you have difficulty falling asleep?
Do you feel that you are excessively sleepy?
What is your sleep-wake schedule during the weekdays/weekends?
How many hours do you sleep per night?
How long does it take you to fall asleep after deciding to go to sleep?
How many times do you wake up during a typical night?
How long does it take you to “get going” after you get out of bed?
Do you snore loudly or stop breathing at night?
Do you have crawling or aching feelings in your legs when trying to fall asleep?
Do you kick or twitch your arms or legs during sleep?
Do you walk in your sleep?
Do you act out your dreams?
Questions regarding daytime behavior are also important, such as the general quality of sleep upon awakening, frequency of daytime napping, and propensity to fall asleep in unacceptable situations such as driving, during conversations, or while watching a movie. It is often crucial to interview the bed partner in addition to the patient to obtain information regarding the patient’s sleep habits; daytime functioning; alcohol, tobacco, and caffeine use; snoring; recent changes in snoring intensity; apnea-like spells; nocturnal spells; morning headaches; confusion; and leg jerks. However, many older adults have no bed partners.
ASSESSMENT OF SLEEP DISORDERS IN THE OLDER PERSON
The polysomnogram is important in the assessment of specific sleep stage abnormalities, leg movements, unusual behaviors, and the presence of underlying sleep-related breathing disorders. The MSLT serves several functions. It is useful in an objective evaluation of sleepiness. It may also reveal narcolepsy, a very rare condition in the older person. The use of video PSG is especially important in the evaluation of parasomnias such as REM sleep behavior disorder (RBD). When patients are suspected of having RBD, it is helpful to place EMG leads on all four limbs during polysomnography.
SLEEP-RELATED BREATHING DISORDER
OBSTRUCTIVE SLEEP APNEA
Sleep-related breathing disorders are probably among the most serious of the sleep disorders. OSA is due to cessation of airflow caused by a complete or partial upper airway collapse at the level of the pharyngeal airways. Central sleep apnea (CSA) is due to cessation of both airflow and respiratory effort. Respiratory events are classified as either complete (apnea) or partial (hypopnea). The respiratory disturbance index (RDI) has been defined as the number of apneas and hypopneas per hour of sleep. At my center, an observation of at least five apneas and hypopneas per hour of sleep is thought to be consistent with a significant level of OSA. However, many older persons without symptoms meet these criteria, and whether they deserve treatment has not yet been well defined.
OSA is due to multiple factors that together can predispose an individual to develop collapse of the airways. Advanced age, neurologic and endocrine impairment, abnormal oral anatomy, obesity, and abnormal nocturnal respiratory reflexes can all contribute to the development of OSA (46,222).
OSA is more common in the older person compared to the young. In individuals >65 years of age, 24% have five or more apneas per hour of sleep, and 81% have >10 respiratory events per hour of sleep (21). A follow-up study from the same group examining a population of community-dwelling geriatric men and women found that those with severe OSA had a significantly shorter survival time on follow-up when compared to those with mild/moderate OSA or minimal/no OSA (19). OSA, however, was not a predictor of death, whereas cardiovascular disease and pulmonary disease were predictors.
Obesity is a central factor contributing to OSA. Although older patients are not as overweight as clinic patients, body mass index (BMI) is still the best predictor of whether an older individual will or will not have OSA (15,21). Elderly patients with OSA have significantly higher BMI compared with patients with minimal or no OSA, supporting the claim that obesity is a risk factor for OSA (19).
Excessive Daytime Sleepiness
EDS is a major symptom in patients with OSA. It is unclear whether the sleepiness is due to disruption of the sleep architecture caused by respiratory-related arousals, repeated episodes of hypoxemia, or factors not yet identified. The EDS may manifest itself as sleepiness during what might be considered inappropriate times. Patients with OSA with EDS report falling asleep while in conversations and while reading, watching television, and even driving.
EDS can also contribute to significant cognitive impairment. OSA is associated with difficulties with attention, memory decline, and concentrating during the day (43). Patients with OSA who experience nocturnal hypoxemia have been shown to possess reduced cognitive functioning (13). Treatment of the underlying sleep-disordered breathing may improve some of the cognitive deficiencies (84). Elderly patients with OSA have also been reported to be at risk for disturbed vigilance, impaired ability to rapidly solve complex problems, and impaired attention/concentration on formal testing of cognition when compared to subjects without OSA (42,102). Nocturnal hypoxemia may also contribute to fatal arrhythmia, hypertension, myocardial infarction, and stroke (223). Other consequences of OSA may include anoxia, cardiorespiratory failure, and ultimately death during sleep (19,24).
SNORING
Snoring may be a hallmark of a sleep-related breathing disorder. Snoring is often disruptive to the sleep of the bed partner who often is first to suspect that there is a problem. Snoring is due to an incomplete upper airway obstruction and is often associated with cardiovascular disease and hypertension (98). Snoring has been linked with hypertension. Research has shown that about one third of patients with hypertension have a sleep-related breathing disorder (12). Repeated or chronic nocturnal hypoxemia may result in impaired cerebral function and hypersomnolence (84).
TREATMENT OF OBSTRUCTIVE SLEEP APNEA
Continuous Positive Airway Pressure and Oral Appliances
Continuous positive airway pressure (CPAP) and sometimes bilevel positive airway pressure (BiPAP) are currently the main methods of treatment. Both work as a splint at the level of the upper airways to prevent their collapse (238,239). Surgery is often an alternative for those who are unable to tolerate CPAP or BiPAP, although it is effective only about 50% of the time. In the elderly, surgery should be considered only if there are no other medical problems that preclude it. Various oral appliances have been recently introduced for the management of mild/moderate OSA. These act by repositioning the mandible and tongue anteriorly (mandibular advancing device and tongue retaining device). The net effect is an improvement in the oropharyngeal airway space (34,156). Oral appliances would not be appropriate for older patients with dentures or for those who are missing a significant number of teeth.
Positional Therapy
Positional therapy may be appropriate for patients with mild OSA confined to supine sleep. Teaching patients to sleep in other positions may be accomplished by sewing a pocket with a tennis ball in the back portion of the pajamas or nightgowns (11).
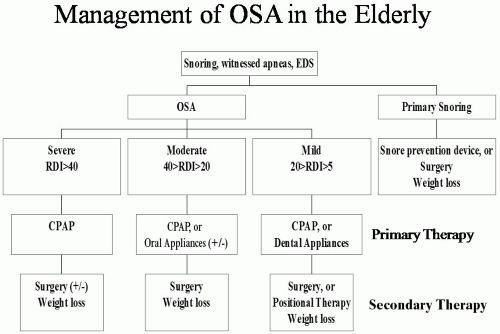
Figure 13-1. Algorithm: potential treatment of OSA in elderly patients. EDS, excessive daytime sleepiness; OSA, obstructive sleep apnea; RDI, respiratory disturbance index; CPAP, continuous positive airway pressure.
Medications
The role of medications such as tricyclic antidepressants, which may increase airway muscle tone and reduce apneas, is somewhat controversial in the elderly because of medication-related side effects and risks of polypharmacy. Previous findings report that medroxyprogesterone may be effective for patients with mild OSA (237).
Surgery
The treatment of OSA in the elderly poses a special problem. Since their sleep is lighter and more disrupted, many patients may not tolerate CPAP very well. Major surgical interventions for OSA, such as bimaxillary advancement, genioglossus advancement, and hyoid suspension, need to be considered with caution, especially if the patient has underlying cardiovascular disease.
Lifestyle
OSA may be potentiated or worsened by a variety of other factors. Many older patients who suffer from insomnia may “self-medicate” themselves with alcohol, which can exacerbate OSA (242). Sleeping in the supine position increases the respiratory disturbances (63). Medications such as benzodiazepines, barbiturates, and narcotics should be used with the utmost care as they may exacerbate respiratory disturbances and reduce a patient’s ability to arouse when an apnea occurs (12). Figure 13-1 outlines a possible algorithm for the management of OSA.
PERIODIC LIMB MOVEMENT DISORDER OF SLEEP
The hallmark of PLMS, also known as nocturnal myoclonus, is a repetitive and continuous leg jerk 0.5 to 5 seconds in duration typically occurring every 20 to 40 seconds during sleep and resulting in arousals (67). The polysomnographic diagnosis of PLMS is made when five or more of these movements are recorded per hour of sleep. Many patients with PLMS present to the clinician with nocturnal leg jerks associated with an uncomfortable sensation and urge to kick or move the involved limb (RLS). Moving the limb often dissipates the uncomfortable sensation. Patients may complain of a motor restlessness, difficulties initiating sleep, and multiple nocturnal awakenings, which result in hypersomnolence (68). Bed partners of patients with PLMS are often bothered by the leg jerks that may not bother the patients themselves. The polysomnogram is often the only reliable way to document the leg movements and thus to make the diagnosis.
RLS is often described as a “creeping” sensation in the lower extremities (41,260,261). This sensation is improved when patients move their legs but returns when the movement ceases. Patients with RLS often complain of difficulty falling asleep. The RLS may be exacerbated by rheumatoid arthritis, excessive caffeine intake, and iron deficiency. Most patients with RLS have PLMS. The converse, however, is not true. Polysomnography is not indicated for making the diagnosis of RLS.
Table 13-1.Medication Chart: Treatment of Restless Leg Syndrome (RLS) in the Older Adult
Drug: Class (generic/brand)
Dose
Potential Side Effects
Iron:
Ferrous Sulfate
325 mg bid/tid with vitamin C 100-200 mg; recommended for ferritin <45 μg/L
Nausea, vomiting, restlessness, constipation; addiction, tolerance may be possible
Darvon (propoxyphene)
65-135 mg at bedtime
Codeine
30 mg
* Only FDA-indicated treatment for moderate-severe restless leg syndrome as of March, 2007.
It is estimated that between 5% and 6% of the population has PLMS. This disorder increases in frequency with older age. One study reported that 45% of older people may have this condition with no gender predilection (20). The diagnosis and treatment of this disorder is extremely important because it can lead to sleep initiation insomnia in the older person. It has been hypothesized that, since dopamine agonists and opiates improve the symptoms of RLS/PLMS, related transmitter systems may be involved in the pathogenesis of these conditions.
PLMS has traditionally been treated with benzodiazepines such as clonazepam or temazepam (171), levodopa/carbidopa (143), or opiates such as acetaminophen and codeine (144). More recently, dopamine agonists such as pramipexole and ropinirole have received approval from the Food and Drug Administration (FDA) for the specific treatment of RLS (110,174,181,206). Table 13-1 outlines the current treatment approaches for patients with PLMS and RLS and possible side effects. Each pharmacologic modality has its advantages and disadvantages. As of today, the benefit-to-risk ratio is unresolved. Recently, iron has been implicated in playing a central role in the physiology of RLS. Iron deficiency can produce RLS symptoms, and iron replacement therapy results in improvement.
Many patients with OSA may also suffer from PLMS. It is prudent that careful analysis be made to determine whether OSA and PLMS coexist in the patient, since treatment of the underlying PLMS (with benzodiazepine) may worsen the OSA. Treatment of the sleep-related breathing disorder may improve or worsen the PLMS; further study of this possibility is needed.
INSOMNIA
Insomnia is the most common sleep complaint reported by older people. It is defined as the inability to either initiate or maintain sleep or as early morning awakening associated with disturbed daytime functioning (178). Older persons are likely to experience sleep maintenance insomnia (difficulty remaining asleep) and early morning awakening (waking early in the morning with the inability to reinitiate sleep). Epidemiologic data have shown a higher prevalence of insomnia in older persons when compared to younger individuals (107,147). In people over 60 years of age, up to 40% may experience insomnia, frequent awakening, and light and disrupted sleep (169).
Insomnia is a symptom, not a diagnosis. When the older person suffers from insomnia, the etiology can be multifactorial. Several factors that should be considered in the differential diagnosis include medical and psychiatric illnesses and polypharmacy. The duration of insomnia—transient (a few days), short term (a few weeks), or chronic (<1 month)— provides important diagnostic information.
In the evaluation of insomnia, a detailed medical and sleep history should be taken. Particular attention should be paid to the underlying medical conditions (heart disease, diabetes), medication use or misuse (polypharmacy), and substance use/misuse (alcohol, caffeine, and/or tobacco). Sleep history should be focused on the sleep hygiene (bedtime, sleep time, wake time). Sleep diaries (sleep logs) are crucial in the evaluation. These self-reported subjective measures allow for easy calculation of total time in bed, total sleep time, and sleep efficiency (116).
Polysomnograms are not necessary in the evaluation of most insomnia. A single PSG may not be representative of a patient’s sleep at home and may not detect insomnia that is not present on a nightly basis (128). However, in the older patient with insomnia, a PSG may be indicated if the clinician suspects an underlying RLS, PLMS, or OSA (90). Others have advocated a formal PSG when traditional therapy of insomnia fails and the possibility of an underlying primary sleep disorder persists (154). Another objectively verifiable indicator of a sleep-wake schedule involves the use of an actigraph, a device worn on the wrist to record body movements (129,209).
There are many causes of insomnia in the older person. The most important group to consider in this age group is patients with insomnia due to medical factors. These factors include primary pulmonary disease [i.e., chronic obstructive pulmonary disease (COPD), asthma], neurologic and neurodegenerative disorders (e.g., parkinsonism, Alzheimer’s disease, cerebrovascular accidents, headaches), nocturia, and pain syndromes. Underlying psychiatric conditions are important contributors to disruption of the sleep architecture. Up to 90% of patients with depression have an abnormal sleep architecture (205). The most striking polysomnographic features of depression include a decreased REM latency and early morning awakening (38).
In addition, older patients may have sleep disruption due to the use/abuse of alcohol, nicotine, and caffeine. In the sleep practice, it is not uncommon to see alcohol being used as a sleeping aid. Although initially it does decrease the sleep latency, it produces arousals, sleep fragmentation, REM deprivation, and REM rebound later during the night. Since the metabolism of alcohol is slower with advanced age, it has more powerful sedating effects (88). Stimulants (caffeine and medications containing stimulants) are notorious causes of insomnia (95). Caffeine is associated with increased sleep latency, reduced sleep efficiency, and spontaneous arousals. Caffeine withdrawal is associated with depression, irritability, and hypersomnolence. Nicotine induces insomnia and sleep fragmentation.
The role of polypharmacy is critical in assessing the older person with sleep disorders. Patients are often treated by multiple physicians who may prescribe several medications. Patients often use over-the-counter medications, vitamins, and herbal preparations.
INSOMNIA TREATMENT
Medications
Pharmacotherapy for insomnia in the older person is common but may be complicated by age-related changes in pharmacodynamics and pharmacokinetics (130). Some sleeping pills, particularly the longer acting ones, have multiple side effects in the older person. These range from hypersomnolence and being accident prone (207) to having disrupted sleep architecture (reduced REM and SWS). Tolerance is a major issue when long-acting sleeping pills are taken chronically, resulting in rebound insomnia and the need of higher dosage to achieve the same clinical efficacy.
Hypnotics
Hypnotics, when used in the older person, need to be given at the lowest possible dose for a short time. Shorter acting hypnotics are preferable, and patients need to be followed up closely. Potential side effects of hypnotics include anterograde amnesia and rebound insomnia. This is true for hypnotics with short or intermediate half-lives. All hypnotics will, if given in appropriate doses, improve insomnia. The goal is to use the medication with the fewest side effects at the lowest dose that will be clinically effective.
Hypnotics, when prescribed to patients with underlying OSA, may produce further nocturnal hypoxemia (115). Withdrawal from hypnotics may actually produce a worsening of insomnia and heightened anxiety. This is especially true with abrupt cessation from longer acting medications. The newer short-acting hypnotics do not have these same side effects and may be safer in the older patient. Examples include zaleplon, which is a nonbenzodiazepine hypnotic from the pyrazolopyrimidine class selective for the benzodiazepine-1 receptor; zolpidem, which is a nonbenzodiazepine hypnotic of the imidazopyridine class selective for the type 1 GABAA-benzodiazepine receptor; and eszopiclone, which is a nonbenzodiazepine agent that is a pyrrolopyrazine derivative of the cyclopyrrolone class (23,87,103,142,164,168). Zolpidem tartrate extended-release tablets have been introduced for the management of sleep maintenance insomnia. The drug consists of a coated two-layer tablet; one layer releases its drug content immediately, and another layer allows a slower release of additional drug content (173,179,185). In 2005, a new melatonin receptor agonist, ramelteon, was made available for the management of sleep initiation insomnia with the advantage of being a nonscheduled agent with zero evidence for abuse or tolerance. This agent selectively binds to the melatonin (MT1 and MT2) receptors in the suprachiasmatic nucleus (SCN), leading to the attenuation of the alerting signal generated by the SNC, which is thought to facilitate the onset of sleep (151,166,186,187). Table 13-2 lists currently available and approved hypnotic agents.
Table 13-2.Medication Chart: Treatment of Insomnia—Newer Hypnotics Agents (as of March, 2007)
Medication
Indication
Half-Life (hr)
Sleep Initiation
Sleep Maintenance
Approved Dose (mg)
Zaleplon
Short-term management of insomnia (improves sleep latency)
1
[check mark]
5, 10
Zolpidem
Short-term management of insomnia (improves sleep latency and increases total sleep time)
2.5
[check mark]
5, 10
Zolpidem CR
Insomnia characterized by difficulties with sleep onset and/or sleep maintenance
2.8
[check mark]
[check mark]
6.25, 12.5
Eszopiclone
Short- and long-term management of insomnia (improves sleep latency and increases total sleep time)
6-7
[check mark]
[check mark]
1, 2, 3
Ramelteon
Insomnia characterized by difficulty with sleep initiation (improves sleep latency and increases total sleep time)
1-2.6
[check mark]
8
Source: Physicians’ Desk Reference. 60th ed. Montvale, NJ: Thomson; 2005:1686-1691;2867-2871;3139-3143;3228-3231.
Sleep Hygiene
Drug therapy alone is not appropriate if one aims to eradicate chronic insomnia. Drug therapy, if used at all, must be combined with educational, behavioral, and cognitive interventions aimed at introducing adaptive behaviors. One of the most important educational approaches for insomnia includes modifying disadvantageous sleep hygiene habits that patients may have adopted over the years (124,127). Originally developed by Hauri (125,126), the basic elements of better sleep hygiene include limiting naps to less than 30 minutes a day, avoiding stimulants and sedatives, limiting liquids at bedtime, keeping a regular sleep schedule, and incorporating light exposure and exercise into the daily routines. Stimulus-control therapy, originally proposed by Bootzin and Nicassio (54), proposes that sleep disturbances are behaviorally conditioned and thus need to be reconditioned. The aim of this intervention is to recondition the bed/bedroom as cues for sleep. Patients are instructed to go to bed only when tired, to get out of bed after 20 minutes of being unable to fall asleep, and to return to bed when sleepy. They are also instructed to avoid looking at the clock, shorten daytime naps, use the bed only for sleep, and get up at a consistent time in the morning (94,95,220).
Sleep restriction therapy proposed by Spielman et al. (229) has in its merits the need to restrict time in bed to provide for better sleep efficiency. This technique involves curtailing time in bed and total sleep time, which may initially lead to a state of sleep deprivation. It works by preventing patients from becoming frustrated by restricting the time spent in bed. Other common therapeutic modalities for insomnia include cognitive intervention, which helps patients gain insight into maladaptive beliefs and attitudes toward sleep, and relaxation techniques and biofeedback, which help patients lower the degree of anxiety and arousal associated with insomnia (54).
CIRCADIAN RHYTHM ABNORMALITIES
The sleep-wake cycle is controlled by the circadian modulator located in the SCN of the anterior hypothalamus. Zeitgebers, external cues such as light, synchronize the circadian rhythms. Disturbances in circadian rhythms are due to a mismatch between the environmental cues and the endogenous circadian rhythms. The hypersomnolence seen in the older person may be due in part to a disintegration of the normal circadian rhythm (136).
Advanced sleep phase syndrome (ASPS) is very common among older patients. Patients with ASPS generally get sleepy early in the evening and wake up early in the morning being unable to reinitiate sleep. Although the older adult may get sleepier in the evening, he/she still tries to remain awake until a “more acceptable” time (e.g., 10:00 or 11:00 PM). Then when they wake up early unable to fall back to sleep, they have not even been in bed long enough to get the sleep they need, resulting in a state of sleep deprivation (10,12). ASPS can be treated with bright light therapy because light is one of the strongest cues for synchronizing circadian rhythms. Bright light therapy involves exposure of 2,500 lux of light at 1 meter eye level. Light exposure in the evening delays sleep initiation (58,59,76).
Melatonin, a neurohormone produced by the pineal gland, can reset sleep onset by synchronization of the internal circadian clock (80). With advanced age, less melatonin is produced (204). Melatonin replacement therapy may be a key for treating insomnia in the elderly. In 1995, Haimov et al. (122) showed a positive correlation between a lower peak level of melatonin and poor sleep efficiency in older patients with insomnia. Melatonin treatment early in the morning may also be used for ASPS. When melatonin is given a few hours prior to the onset of the endogenous production (which peaks around 3:00 to 5:00 AM), it will shift the circadian pacemaker to an earlier time and thus cause a phase advance (152,153,227). Currently, more data are needed to improve our understanding of the appropriate dosage, pharmacologic properties, and indications. More data are also needed regarding the appropriate safety and efficacy of this substance. Since the FDA does not regulate melatonin, care must be exercised when using it.
SLEEP DISORDERS IN NEUROLOGIC DISORDERS
Patients with a history of dementia may have a number of underlying sleep disturbances consisting of insomnia, hypersomnia, circadian rhythm disturbances, excessive motor activity at night, nocturnal agitation, and wandering and abnormal nocturnal behaviors (64). Dementia patients with sleep problems may be at increased risk for irritability, impaired motor and cognitive skills, depression, and fatigue (39). Patients with dementia are also at risk for additional sleep disturbances, such as OSA and PLMS, which occur at a higher incidence with aging. Many of these sleep disruptions can cause considerable caregiver burden and may put the patient at increased risk for institutionalization in nursing home facilities (155,197).
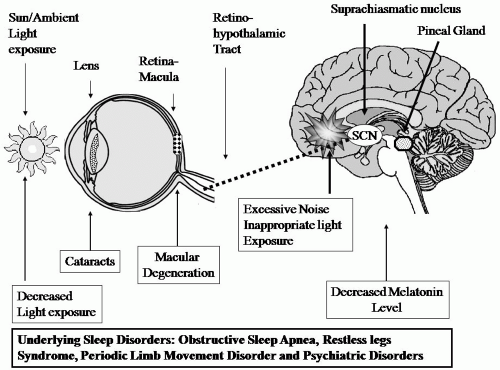
Sleep disturbances in dementia may be due to both underlying direct and indirect mechanisms (39,64). Direct mechanisms are related to specific lesions in the neuroanatomic pathways involved in sleep physiology and neurochemistry. Structural alteration of the sleep-wake-generating neurons located in the SCN is one example of the direct mechanism, whereas insufficient light exposure and excessive noise at the patient’s living quarters are examples of the indirect or external mechanisms that disturb sleep (Fig. 13-2).
ALZHEIMER’S DISEASE
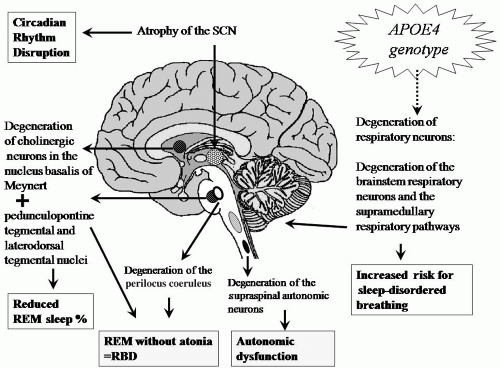
In Alzheimer’s disease (AD), degeneration of the neurons of the SCN may be responsible for circadian rhythm abnormalities, sundowning syndrome, and other sleep-wake schedule disturbances (Fig. 13-3) (39,64). The severity of circadian rhythm disturbances is shown to be correlated with the severity of dementia (17,18). Sleep studies in patients with dementia demonstrate decreased sleep efficiency, increased diffuse slow-wave activity, and reversal of their circadian rhythmicity, which, after incontinence, is the second most common cause for institutionalization (196).
Degeneration of the cholinergic neurons in the nucleus basalis of Meynert, the pedunculopontine tegmental and laterodorsal tegmental nuclei, and noradrenergic neurons of the brainstem may be responsible for the predictable decreased REM sleep in AD patients (Fig. 13-3) (39,64). Degeneration of the brainstem respiratory neurons and the supramedullary respiratory pathways may cause sleep apnea and other respiratory dysrhythmias in sleep in AD (Fig. 13-3) (39,64).
Indirect mechanisms include pharmacologically related side effects, underlying psychiatric diagnosis such as mood disorders, increasing incidence of PLMS in elderly AD patients, and age-related alterations in sleep (Fig. 13-2). Other indirect mechanisms include general medical diseases affecting the cardiorespiratory system and environmental factors such as insufficient light and excessive environmental noise in nursing homes facilities or other long-term care institutions (Fig. 13-2).
Figure 13-2. Pathophysiology of sleep disturbances in patients with dementia: potential external and intrinsic factors. (Modified from Avidan A. Sleep in dementia and other neurodegenerative disorders. In: Culebras A, ed. Sleep disorders and neurologic diseases. 2nd ed. New York: Taylor & Francis Group; 2007.)
Sleep Architecture in Alzheimer’s Disease
Patients with AD have dramatic sleep architectural abnormalities. The signature findings include decrease in sleep efficiency, increase in NREM stage 1 sleep, increase in arousal and awakening frequency, and a reduction in total sleep time, sleep spindles, and K-complexes. A profound disruption in sleep-wake rhythmicity occurs primarily early in the onset of AD. Sleep fragmentation subsequently leads to hypersomnolence (increased daytime sleepiness), nocturnal insomnia, nocturnal wandering, increase in cognitive decline, increase in the number of daytime naps, increase in time in bed and time spent awake in bed, increase in the frequency of nocturnal wandering, disorientation, and confusion (47,64,255, 256, 257, 258 and 259).
Later on, as AD progresses, patients may present with a more dramatic reduction of REM sleep, increased REM sleep latency, and a marked alteration of the circadian rhythm resulting in hypersomnolence (39). In fact, sleep and cognitive dysfunction are positively correlated in AD. Patients with AD are also susceptible to “sundowning,” a term describing the nocturnal exacerbation of agitation or disruptive behavior in older patients (248). Sundowning is frequently encountered in dementia and remains a frequent cause of institutionalization in patients with AD. Inevitably, the medications often used to treat AD also affect sleep. Current pharmacotherapy for cognitive loss in AD involves the use of cholinesterase inhibitors, which may increase REM sleep and may also induce insomnia and vivid dreams (45).
Circadian Rhythm Disturbances in Alzheimer’s Disease
The symptoms of insomnia and hypersomnia can reflect a primary circadian dysrhythmia. AD patients tend to sleep more during the day and be more active during the night. This increased motor activity at night is the major contributing factor to significant caregiver distress.
Direct mechanisms thought to contribute to circadian dysrhythmia in patients with AD and other dementing conditions are related to degenerative changes that take place in the SCN and to decreased melatonin production in the pineal gland (Figs. 13-1 and 13-2) (75,236,240,241). Indirect mechanisms include medications prescribed for these patients that cause nocturnal confusion, or sundowning. AD patients are commonly affected by the irregular sleep-wake rhythm (ISWR), which is characterized by a lack of discernable sleep-wake circadian rhythm. Instead of having a major sleep period, sleep is fragmented into three or more periods during the 24-hour day, with the longest sleep period occurring between 2:00 and 6:00 AM. Patients with ISWR may present with hypersomnia, insomnia, or the need for frequent naps throughout the day. The disorder also affects the sleep quality of the caregiver.
Figure 13-3. Pathophysiology of sleep disturbances in neurodegenerative disorders: direct mechanisms. RBD, REM sleep behavior disorder; SCN, suprachiasmatic nucleus; (broken arrow) demonstrates a hypothetical relationship (Modified from Avidan A. Sleep in dementia and other neurodegenerative disorders. In: Culebras A, ed. Sleep disorders and neurologic diseases. 2nd ed. New York: Taylor & Francis Group; 2007.)
Important factors that may contribute to ISWR include weak external entraining stimuli such as reduced exposure to environmental light and diminished daytime activity. The diagnosis of ISWR is made by reviewing the patient’s sleep log or actigraphy confirming the lack of periodic circadian rhythmicity. A history of isolation or reclusion may aid in diagnosis. The differential diagnosis of ISWR includes other sleep or psychiatric disorders that can cause fragmented sleep, poor sleep hygiene, and voluntary maintenance of irregular sleep schedules.
Sleep Disordered Breathing in Alzheimer’s Disease
Sleep-related breathing disorders, such as OSA, are very common in AD patients compared to nondemented elderly and to younger adults (93,131). One study demonstrated that the severity of AD is proportional to the severity of the OSA (16,137). Furthermore, anecdotal reports of dementia-like symptoms associated with OSA have led to the speculation that there may be a causal relationship between sleep-disordered breathing and AD (219).
In AD, sleep apnea could be a consequence of cell loss in the brainstem respiratory center. Conversely, neuronal degradation in AD may be hastened by nightly insults of intermittent cerebral hypoxemia related to the underlying OSA. One of the key genotypic markers for AD is the apolipoprotein E epsilon 4 (APOE4) allele. A recent discovery that sleep-disordered breathing (SDB) is associated with the APOE4 allele in the general population has sparked an interest in this topic because OSA is characterized by multiple genetic vulnerabilities (44,141). In individuals under age 65, the APOE4 allele was more significantly associated with increased risk of OSA (201). However, other studies did not replicate the result in part because of different genetic populations and different age cohorts (106,208). In a recent study of 1,775 participants aged 40 to 100 years with an OSA prevalence rate of 19%, after adjustment for age, sex, and BMI, the presence of any APOE4 allele was associated with increased odds of having OSA (120).
Only gold members can continue reading. Log In or Register to continue