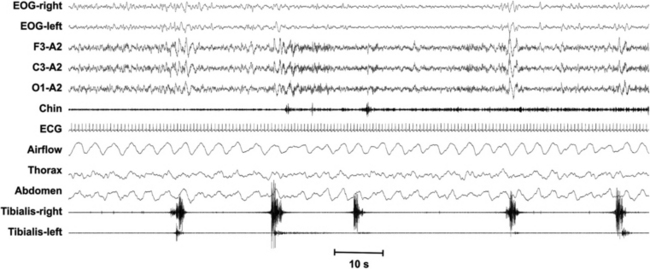
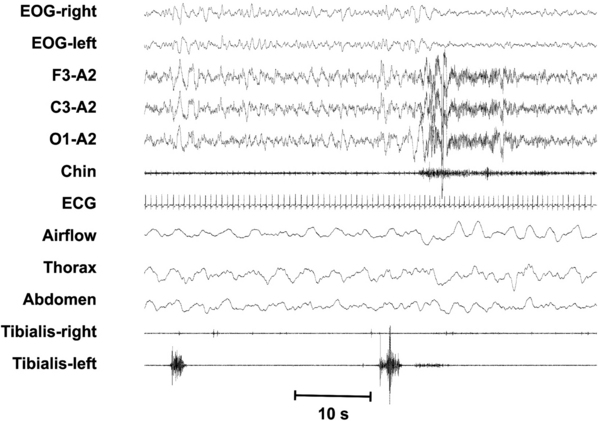
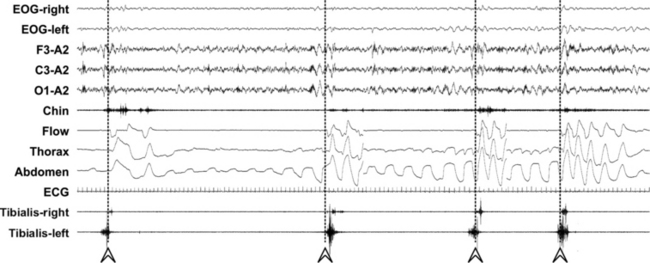
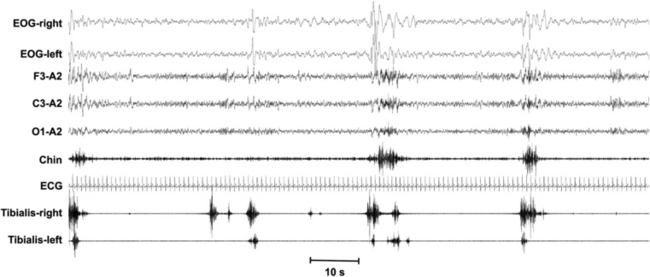
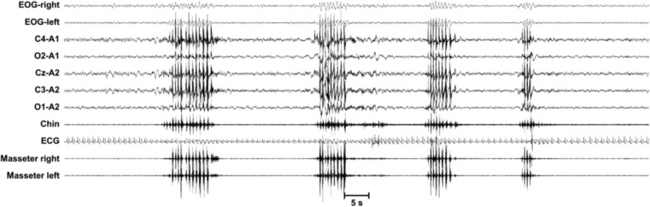
Chapter 7 This chapter focuses on scoring techniques of sleep-related movement disorders. FIGURE 7.1 Periodic limb movements (PLM) are movements lasting 0.5 to 10 seconds, separated by 5 to 90 seconds (onset to onset), and occurring in a series of at least four, with a minimum amplitude of an 8-μV increase in electromyographic (EMG) voltage above resting EMG. The number of the movements presenting these features per hour defines the PLM index. It can be calculated during sleep or during wakefulness. FIGURE 7.2 A leg movement is considered associated with an arousal when there is less than 0.5 seconds between the end of one event and the onset of the other, regardless of which is first. The periodic limb movements (PLM)/arousal index is the number of PLM events associated with arousal per hour of sleep. FIGURE 7.3 A leg movement is associated with the ending of an apnea/hypopnea event when they overlap or the offset of the earlier event precedes the onset of the other by less than 0.5 seconds, regardless of which is first; these leg movements are excluded from the computation of periodic limb movements–related parameters. Arrowheads and dashed lines indicate the resumption of breathing after apnea episodes. FIGURE 7.4 The leg motor activity during sleep also contains irregular short-interval movements interrupting the regular periodic sequences. Also long-interval movements (>90 seconds) are present that do not belong to the periodic activity. The degree of periodicity can be measured by means of the periodicity index (the number of movements in sequences of at least four separated by 10 to 90 seconds divided by the total number of movements, including those with intervals <10 seconds and >90 seconds). Note that for this analysis intervals of less than 5 seconds are also counted, in contrast to that for periodic limb movements index. FIGURE 7.5 Polysomnographic recording of a sequence of rhythmical masticatory muscle activity (RMMA; at least three rhythmical phasic contractions at a frequency of 1 Hz, lasting between 0.25 and 2 seconds) episodes in one subject with sleep bruxism (SB). An episode of SB may consist of RMMA, tonic (sustained contraction for more than 2 seconds), or mixed phasic-tonic masticatory muscle activities, associated with tooth-grinding sound during sleep. Contractions shorter than 0.25 seconds are scored as myoclonus. Each SB episode has to be separated by a period of at least 3 seconds of stable background electromyogram (EMG) to be scored as a new SB episode. SB can be scored reliably by audio-video recording in combination with polysomnography, with a minimum of two audible tooth-grinding episodes per night, in the absence of epilepsy. The diagnosis of SB requires the presence of at least four episodes of SB per hour of sleep or at least 25 individual masticatory muscle bursts per hour of sleep, accompanied by at least two audible episodes of tooth-grinding noise. For the scoring of SB the recommended chin EMG electrodes have been indicated to be sufficient, but additional masseter and/or temporal EMG can be helpful, in accordance with the discretion of the investigator or clinician.
Sleep-Related Movements and Scoring Techniques
Related posts:
 1: Narcolepsy—Unequivocal Diagnosis After Split-Screen, Video-Polysomnographic Analysis of a Prolonged Cataplectic Attack
1: Narcolepsy—Unequivocal Diagnosis After Split-Screen, Video-Polysomnographic Analysis of a Prolonged Cataplectic Attack
 4: Isolated Sleep Paralysis: An REM-“Sleep” Polysomnographic Phenomenon as Documented With Simultaneous Clinical and Electrophysiological Assessment
4: Isolated Sleep Paralysis: An REM-“Sleep” Polysomnographic Phenomenon as Documented With Simultaneous Clinical and Electrophysiological Assessment
 Motor Disorders During Sleep
Motor Disorders During Sleep
 Oral Appliances and Surgical Techniques for Obstructive Sleep Apnea Syndrome Therapy
Oral Appliances and Surgical Techniques for Obstructive Sleep Apnea Syndrome Therapy
 Specialized Techniques
Specialized Techniques



