Somatosensory Evoked Potentials
QUESTIONS
1. Somatosensory evoked potentials are best recorded by using an amplification of:
A. 100
B. 1,000
C. 10,000
D. 100,000
View Answer
1. (D): Averaging in evoked potential testing increases the signal-to-noise ratio. An amplification of 100,000 is needed to improve the signal-to-noise ratio. (Chiappa 1997, p. 288)
2. Somatosensory evoked potentials are best recorded using a low-frequency filter of:
A. 30 Hz
B. 3 Hz
C. 50 Hz
D. 5 Hz
View Answer
2. (A): Low-frequency filter of 30 Hz is appropriate to record SSEP. This frequency cutoff will filter movement artifact encountered during the recordings. (Chiappa 1997, p. 288)
3. Somatosensory evoked potentials are best recorded by using a high-frequency filter of:
A. 100 Hz
B. 1,000 Hz
C. 3,000 Hz
D. 30,000 Hz
View Answer
3. (C): A high-frequency filter of 3,000 Hz is most appropriate for recording SSEP. (Chiappa 1997, p. 288)
4. Somatosensory evoked potentials are best recorded by using a sweep duration of:
A. 10 ms
B. 20 ms
C. 200 ms
D. 100 ms
View Answer
4. (D): Sweep duration of 100 ms is needed to record SSEP. Also, the dwell time should be set at 0.2 ms. (Chiappa 1997, p. 288)
5. Erb’s point N9 is the reference point for latency measurement. It corresponds to:
A. Cervicomedullary junction
B. Cauda equina
C. Brachial plexus
D. Cubital fossa
View Answer
5. (C): The N9 of the somatosensory evoked potential originates in the brachial plexus. Cauda equina potential corresponds to N21. N11/13 complex corresponds to cervicomedullary junction. Cubital fosse potentials are not used in SSEP in clinical practice. (Chiappa 1997, p. 288)
6. N11-13 complex corresponds to:
A. Cervicomedullary junction
B. Cauda equine
C. Brachial plexus
D. Cubital fossa
View Answer
6. (A): The N9 of the somatosensory evoked potential originates in the brachial plexus. Cauda equina potential corresponds to N21. N11/13 complex corresponds to cervicomedullary junction. Cubital fosse potentials are not used in SSEP in clinical practice. (Chiappa 1997, pp. 289-290)
7. N20 shown in the Figure 10.1 corresponds to:
A. Cervicomedullary junction
B. Cauda equine
C. Thalamus
D. Cubital fossa
View Answer
7. (C): The N9 of the somatosensory evoked potential originates in the brachial plexus. Cauda equina potential corresponds to N21. N11/13 complex corresponds to cervicomedullary junction. Cubital fosse potentials are not used in SSEP in clinical practice. N20 corresponds to thalamic action potential. (Chiappa 1997, pp. 289-290)
8. Somatosensory evoked potential (SSEP) in lower extremity is commonly done using posterior tibial nerve compared to common peroneal nerve at the knee because:
A. Posterior tibial nerve stimulation has high threshold for stimulation
B. Posterior tibial nerve stimulation produce higher amplitude lumbar potentials
C. Posterior tibial nerve is a pure sensory nerve
D. All of the above
View Answer
8. (B): Stimulation of posterior tibial nerve at ankle produces higher amplitude of lumbar and scalp potentials than stimulation of common peroneal nerve. This amplitude difference is possibly due to rich innervation of the sole of the foot. (Chiappa 1997, p. 294)
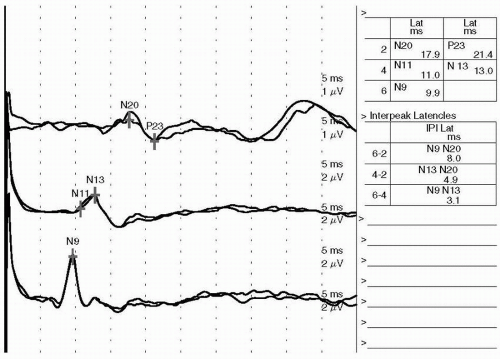 Figure 10.1. Somatosensory evoked potential (SSEP) median |
9. SSEP tests the integrity of:
A. Corticospinal tract
B. Spinothalamic tract
C. Spinocerebellar tract
D. Dorsal column
View Answer
9. (D): SSEP only tests the integrity of myelinated large fibers sensory system, that is, dorsal column. At times, SSEP may be completely normal if the lesion involves the anterior two third of the spinal cord and spares dorsal column. (Chiappa 1997, p. 319)
10. The most common problem encountered with the SSEP test is excessive muscle activity.
A. False
B. True
View Answer
10. (B): Muscle artifact is the most common problem encountered. It is very crucial that patient relaxes during the testing. If the problem persists, a short acting hypnotic can be given to improve signal-to-noise ratio. (Chiappa 1997, p. 303)
11. The SSEP stimulus intensity should be enough to produce muscle twitch.
A. True
B. False
View Answer
11. (A): SSEP stimulus intensity should be enough to produce a muscle twitch. Inadequate stimulation of the tibial nerve sometimes results in delayed responses. (Chiappa 1997, p. 303)
12. If the SSEP stimulus intensity is low, the scalp potentials will be affected as follows:
A. Responses will have a low amplitude
B. Responses will have a high amplitude
C. Responses will have a short latency
D. Responses will have a prolonged latency
View Answer
12. (D): If stimulus intensity is increased, the responses’ latency will become normal. SSEP stimulus intensity should be enough to produce a muscle twitch. Inadequate stimulation of the tibial nerve sometimes results in delayed responses. (Chiappa 1997, p. 306)
13. In SSEP, bilateral stimulation is not used in clinical practice because:
A. Amplitude of responses will be low
B. Responses will be delayed
C. Normal responses from the good side will mask the abnormality on the bad side
D. None of the above
View Answer
13. (C): SSEP bilateral stimulation is not used in clinical practice because of normal responses from good side will mask the abnormality on the bad side. The only possible use for bilateral stimulation in SSEP testing may be for obtaining a larger amplitude response when using the lower limb SSEP to monitor spinal cord functioning during surgery. (Chiappa 1997, p. 306)
14. Bilateral stimulation is used in the following situation:
A. To monitor spinal cord functioning during surgery
B. To evaluate brain death
C. To evaluate multiple sclerosis
D. A and B
View Answer




14. (C): Bilateral absence of cortical responses (N20) on median somatosensory evoked potential is associated with a poor outcome in comatose patients. The studies suggest that if a comatose patient is missing cortical responses bilaterally, then that patient’s outcome will be a persistent vegetative state at best. (Chiappa 1997, p. 389)
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
