Specific developmental disorders in childhood and adolescence
Specific developmental disorders in childhood and adolescence
Helmut Remschmidt
Gerd Schulte-Körne
Introduction
The term ‘specific developmental disorders’ includes a variety of severe and persistent difficulties in spoken language, spelling, reading, arithmetic, and motor function. Skills are substantially below the expected level in terms of chronological age, measured intelligence, and age-appropriate education and cannot be explained by any obvious neurological disorder or any specific adverse psychosocial or family circumstances. As the deficits are quite substantial, analogies were initially made to neurological concepts and disorders such as word-blindness, alexia, aphasia, and apraxia, thus giving rise to the notion that neurological deficits are the aetiological basis of these disorders. Since this could not be demonstrated, the next step was to define the disorders in a more functional way, taking into account not only psychometric testing but also psychosocial risk factors and the quality of schooling and education.
Table 9.2.2.1 Specific developmental disorders: a comparison of ICD-10 and DSM-IV NOS, not otherwise specified
ICD-10
DSM-IV
Specific developmental disorders of speech and language (F80)
Communication disorders
Specific speech articulation disorder (F80.0)
Expressive language disorder (315.31)
Expressive language disorder (F80.1)
Mixed receptive-expressive language disorder (315.31)
Receptive language disorder (F80.2)
Phonological disorder (315.39)
Acquired aphasia with epilepsy (Landau-Kleffner syndrome) (F80.3)
Stuttering (307.0)
Other developmental disorders of speech and language (F80.8)
Communication disorder NOS (307.9)
Specific developmental disorders of scholastic skills (F81)
Learning disorders
Specific reading disorder (F81.0)
Reading disorder (315.00)
Specific spelling disorder (F81.1)
Mathematics disorder (315.1)
Specific disorder of arithmetical skills (F81.2)
Disorder of written expression (315.2)
Specific disorder of scholastic skills (F81.3)
Learning disorder NOS (315.9)
Other developmental disorders of scholastic skills (F81.8)
Specific developmental disorder of motor function (F82)
Motor skills disorder
Developmental co-ordination disorder (315.4)
Mixed specific developmental disorders (F83)
Today, numerous findings support the validity of the diagnostic concept of specific developmental disorders. These disorders and pervasive developmental disorders have the following features in common (ICD-10)(1):
An onset that invariably appears during infancy or childhood.
An impairment or delay in the development of functions that are strongly related to biological maturation of the central nervous system.
A steady course that does not involve the remissions and relapses that tend to be characteristic of many mental disorders.
Thus the term ‘specific developmental disorders’ reflects the fact that the deficits are circumscribed and relatively isolated against the background of an otherwise undisturbed psychological functioning.
Classification
In the multiaxial classification of child and adolescent psychiatric disorders,(2) specific developmental disorders are classified on the second axis named ‘Specific disorders of psychological development’, whereas pervasive developmental disorders are classified on the first axis (clinical psychiatric syndromes).
Based on the history and course of the disorders, two types can be distinguished:
Disorders in which a phase of previously normal development has occurred prior to manifestation of the disorder. This, for example, applies to the Landau-Kleffner syndrome.
An additional condition in which the abnormality was present from birth. This is especially true for autism. Autism is classified in the category ‘pervasive developmental disorders’, which are discussed elsewhere.
In DSM-IV,(3) nomenclature is somewhat different, but generally includes disorders identical or similar to those in ICD-10. In DSM-IV, ‘communication disorders’ correspond to ‘specific developmental disorders of speech and language’. However, they also include stuttering, which is not included in the corresponding category of ICD-10.
‘Learning disorders’ (DSM-IV) is the category that corresponds to specific developmental disorders of scholastic skills, and ‘motor skills disorder’ to ‘specific disorders of motor function’.
Table 9.2.2.1 shows the terminology used in both classification systems. The headlines of the two systems correspond; however, the subcategories show some differences.
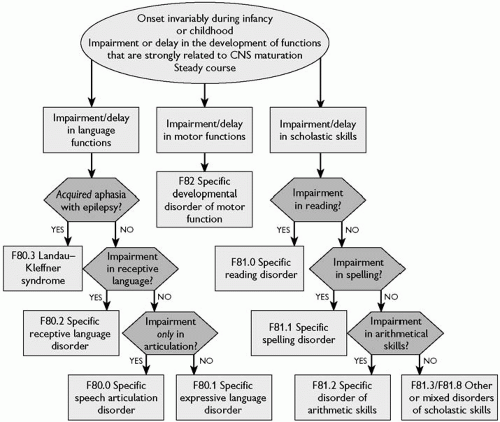
Figure 9.2.2.1 shows a decision tree which includes the three main areas of dysfunction and addresses diagnosis and differential diagnosis.
Specific developmental disorders of speech and language
The main characteristic of these disorders is a disturbance of language acquisition from the early stages of development. The disturbance, however, is not directly attributable to neurological or speech mechanism abnormalities, sensory impairments, intellectual disability, or environmental factors.(1)
There are three main problems in distinguishing these disorders from the normal state and other conditions:
1 Differentiation from the normal state: the disorders must be distinguished from normal speech and language development, bearing in mind the great variations seen in the normal pattern. To make the diagnosis, the disorder must clearly be clinically significant, which can be determined by four main criteria: severity, course, pattern, and associated problems.
2 Differentiation from intellectual disability (mental retardation): the degree of speech and language dysfunction must always be considered with respect to the child’s cognitive level.
3 Differentiation from disorders due to sensory impairment or impairments of the central nervous systems: speech and language disorders resulting from severe deafness, specific neurological impairments, or structural brain abnormalities are not classified in the category of specific developmental disorders of speech and language.
Fig. 9.2.2.1 Specific developmental disorders. CNS, central nervous system.
Specific speech articulation disorder
(a) Clinical features
The main feature of the disorder is the child’s failure to use speech sounds appropriate for his or her mental age, while other language skills are within the normal range. Difficulties include errors in sound production and use, especially substitution of one sound for another. Difficulties in speech sound production usually interfere either with academic achievement or social communication. There are several degrees of severity reaching from mild or no impairment of speech intelligibility to completely incomprehensible speech. Sound substitutions are considered less severe than sound omissions. The sounds most frequently misarticulated are those acquired later during speech development (l, r, s, z, th, ch). However, consonants and vowels that range early in the development sequence may be affected in younger children.
It is very important to relate the misarticulations to normal development. At the age of 4 years, errors in speech and sound production are very frequent, but children are usually understood even by strangers. At 6 to 7 years of age, most speech sounds can be adequately reproduced, and by the age of 11 to 12, children should be capable of almost all speech sounds.
(b) Classification
In ICD-10, speech articulation disorder (F80.0) is classified in the category ‘Specific developmental disorders of speech and language’. The counterpart in DSM-IV is the category ‘Phonological disorder’ (315.39), classified in the category ‘Communication disorders’ (see Table 9.2.2.1).
(c) Diagnosis and differential diagnosis
The leading feature, the age-appropriate misarticulation of speech sounds with the result that others have difficulties in understanding the child, usually allows one to diagnose the disorder. There are three types of symptoms that can be observed: substitutions, omissions, and distortions of speech sounds. The diagnosis should only be made if the severity of misarticulation is outside the limits of the normal variation for the child’s mental age. Further requirements are that non-verbal intelligence and expressive and receptive language skills should be within the normal range.
Differential diagnoses include intellectual disability, hearing impairment, or other sensory deficits or severe environmental deprivation.
(d) Epidemiology
Moderate to severe developmental articulation disorders can be found in 2 to 3 per cent of 6- and 7-year-old children, with less severe disorders even more frequent. The frequency of occurrence falls to 0.5 per cent by the time children are 17 years old (DSM-IV).
(e) Aetiology
As it has been demonstrated that the disorder runs in families, it is assumed that genetic factors are important for its manifestation.
(f) Course and prognosis
The prognosis is favourable if no other associated features such as hearing impairment, neurological conditions, cognitive impairments, or psychosocial problems are present. However, the course varies depending on the severity and the above-mentioned associated features.
(g) Treatment
Treatment is necessary and appropriate if the child is handicapped in his or her everyday life and cannot be understood by parents, siblings, or other persons. The focus of the therapy depends on whether speech articulation disorder is an isolated phenomenon or if other impairments or dysfunctions are present (e.g. developmental disorder of motor functions). If it is an isolated phenomenon, functional speech therapy can be carried out on the principle that mispronounced sounds should not be repeated when correcting them, but substituted by the correctly pronounced sound.(4) It is advisable to carry out this kind of therapy before the child enters school. If other disorders are present, a comprehensive therapeutic programme that includes speech therapy needs to be developed.
Expressive language disorder
(a) Clinical features and classification
The main feature of this disorder is that the child’s ability to use expressive spoken language is reduced below the mental age appropriate level, while language comprehension ranges within normal limits. Abnormalities in articulation may co-occur.
In ICD-10, the following symptoms are considered important for diagnosis (ICD-10, p. 237)(1):
delay of the development of expressive language (e.g. absence of single words by the age of 2 years, failure to generate simple two-word sentences by 3 years)
restricted vocabulary development
overuse of a small set of general words
difficulties in selecting appropriate words and word substitutions
short utterance length and immature sentence structure
syntactical errors, especially omissions of word endings or prefix
misuse of or failure to use grammatical features such as prepositions, pronouns, articles, and verb and noun inflexions.
The DSM-IV criteria requires measures of expressive language development being substantially below those obtained from standardized measures of both non-verbal intellectual capacity and receptive language development, interference with academic or occupational achievement, and the exclusion of mixed receptive-expressive disorder and pervasive developmental disorders.
(b) Diagnosis and differential diagnosis
The diagnosis is made by clinical observation, with special emphasis on expressive language functions and the use of individually administered standardized tests of expressive language. The differential diagnosis should rule out mixed receptive-expressive language disorder (DSM-IV), characterized by an impairment of receptive language functions. Autistic disorder may also involve expressed language impairment, but autism can be distinguished by characteristic communication impairments. Finally, intellectual disability and sensory impairments (e.g. hearing impairment or other sensory deficits) need to be ruled out, as well as severe environmental deprivation. The diagnosis is confirmed using intelligence tests, audiometric tests, neurological investigations, and a careful history. Finally, acquired aphasia needs to be ruled out. This can be done by assessing any medical condition that may have caused the disorder.
(c) Epidemiology
In the absence of thorough epidemiological studies, estimates suggest that between approximately 3 and 5 per cent of children may be affected by expressive language disorder of the developmental type. The acquired type seems to be less common.
(d) Aetiology
DSM-IV distinguishes two types of expressive language disorders: the developmental type and the acquired type. In the developmental type, impairment of expressive language begins at a very early age and is not associated with neurological factors, while the acquired type occurs after a period of normal development and is caused by neurological or general medical conditions (e.g. head trauma, encephalitis). It is assumed that the developmental type is caused by genetic factors that influence language development.
(e) Course and prognosis
The course depends on the type of disorder (developmental or acquired type) and severity. Usually, the disorder can be diagnosed by the age of 3 years, while milder forms are often only detected later. According to DSM-IV,(3) approximately half of the children appear to outgrow the developmental type of expressive language disorder, while the other half have persistent difficulties. The outcome of the acquired type depends on the severity and location of the brain pathology.
(f) Treatment
As causal treatment is not possible, treatment measures are based on general principles that have been found to be useful and effective in clinical practice.
1 The first step is to explain clearly to parents the nature of the disorder and the fact that several other disturbances manifested by the child may be a result of the child’s communication deficit.
2 The best time to commence speech therapy depends upon the severity of the disorder, the child’s cognitive and motivational structure, and other disorders that might be present. Instead of treating children too early (e.g. before the age of 3 years), offering advice and guidance to the parents is extremely important.
3 Treatment itself concentrates on teaching language skills using techniques such as imitation and modelling. The therapist should focus interventions selectively on the areas of difficulty, thus increasing the child’s phonological repertoire. Non-verbal communication techniques may be used if verbal communication is substantially impaired. But the therapist should always make sure that non-verbal communication does not dominate the verbal one.
4 In therapeutic programmes, everyday situations are now preferred to very structured programmes. This is because many therapists found that therapeutic progress during sessions was not transferred to everyday life situations. During structured treatment sessions the children are taught to give correct answers to questions that have nothing to do with their situation in everyday life, and it is now thought that structured language training may prevent them using language according to their needs.(5)
5 Alternative communication, such as sign language, should only be used if the child suffers from severe auditory comprehension deficits. The use of a sign language, however, is no longer regarded as an obstacle to the improvement of expressive language skills.(6)
Receptive language disorder
(a) Clinical features and classification
This disorder is characterized by the child’s inability or reduced ability to understand language in a way appropriate for his or her mental age. As expressive language production depends on language comprehension; expressive language is also profoundly disturbed and abnormalities in word-sound production can be observed.
The diagnostic guidelines of ICD-10 include the following features:
failure to respond to familiar names (in the absence of non-verbal clues) by the first birthday
inability to identify at least a few common objects by 18 months
failure to follow simple, routine instructions by the age of 2 years
inability to understand grammatical structures (e.g. questions, comparatives)
lack of understanding of the more subtle aspects of language (tone of voice, gestures, etc.).
Owing to the disturbances in both receptive and expressive functions, the disorder is called ‘receptive-expressive language disorder’ in DSM-IV. The diagnostic criteria require scores of both receptive and expressive language development substantially below those obtained from standardized measures of non-verbal intellectual capacity, interference with academic or occupational achievement, and exclusion of pervasive developmental disorders.
(b) Diagnosis and differential diagnosis
Diagnosis is based on three factors: a careful history taken from the child’s parents, a thorough clinical investigation including neurological assessment and detailed speech and language assessment, and standardized tests measuring expressive and receptive language functions.
Differential diagnosis should rule out expressive language disorder (which is the case in the presence of language comprehension), specific speech articulation disorder, in which the receptive and expressive language functions are unimpaired, autism (which can be distinguished by the typical communication disturbance), intellectual disability, sensory deficits, and severe environmental deprivation. These disorders can be excluded by intelligence tests, audiometric tests, neurological investigations, and taking a history.
(c) Epidemiology
Owing to the absence of epidemiological studies, the frequency with which the disorder occurs can only be estimated. According to estimations, the disorder occurs in up to 3 per cent of school-age children and is probably less common than expressive language disorder.
(d) Aetiology
As in other developmental language disorders, there is evidence that genetic factors play the most important role in aetiology.(7) The frequent association of disturbed language acquisition with adverse psychosocial factors in the family does not contradict a primarily genetic cause, as many children who grow up under these circumstances show entirely normal developmental patterns of speech and language skills.(8)
(e) Course and prognosis
The long-term prognosis is poor. Only half the patients in the sample studied by Rutter et al.(9) had normal conversational skills when they were in their twenties, and there was a decline in non-verbal IQ from childhood to adulthood. The course again depends on the type (developmental or acquired) and severity of the disorder. The disorder is usually detected before the age of 4 years, but earlier in severe cases. The prognosis is poorer than in expressive language disorder. As far as the acquired type is concerned, the prognosis varies depending on severity, location of brain pathology, the child’s age, and the level of language development prior to the disorder.
(f) Treatment
Treatment is generally undertaken along the same lines as in expressive language disorders. However, owing to the nature of the disorder, all factors that facilitate language comprehension should especially be encouraged. Non-verbal forms of communication such as sign language can be helpful.
Acquired aphasia with epilepsy (Landau-Kleffner syndrome)
(a) Clinical features and classification
The Landau-Kleffner syndrome is a rare disorder characterized by receptive and expressive language impairment and epileptic seizures, but retained general intelligence, and manifestation after a period of normal development, including language development. The onset of the disorder typically occurs between 3 and 7 years of age and is accompanied by paroxysmal electroencephalographic abnormalities, mainly bilateral spikes in the posterior temporal and parietal regions and epileptic seizures in about 80 per cent of cases.(10) The loss of language may occur gradually over a period of months or abruptly within a few days or weeks.
Aphasia usually starts with receptive language problems occurring together with the characteristic electroencephalographic changes, followed by expressive language difficulties. Usually, the first sign is the impairment of receptive language functions with difficulties in auditory comprehension. During the manifestation period, symptomatology is variable: some children become mute, others express jargon-like sounds, and some produce misarticulations and have difficulties in word fluency. During the manifestation period, emotional and behavioural symptoms are common; they can be regarded as a reaction to the loss of language functions and appear as anxiety reactions, acting-out behaviour, and aggression.
In DSM-IV, the condition is classified in the category mixed receptive-expressive language disorder, acquired type.
(b) Diagnosis and differential diagnosis
The diagnosis can be based upon a detailed history of the child’s development, assessment of language functions, careful neurological assessment, and by electroencephalography. The differential diagnosis includes other types of acquired aphasia without epileptic seizures and electroencephalographic abnormalities, and disintegrative disorders of childhood such as dementia infantilis Heller (Heller’s syndrome) (see Chapter 9.2.2).
Only gold members can continue reading. Log In or Register to continue