♦ Preoperative
Operative Planning
- Review imaging studies
- Non-contrast head computed tomography (CT) essential for precise localization of subdural hematoma (SDH); most often located at the frontotemporo-parietal convexity from bleeding of injured parasagittal or cortical veins
- Adjust window on CT scan to detect chronic appearing SDH, which may have similar density to brain
- Non-contrast head computed tomography (CT) essential for precise localization of subdural hematoma (SDH); most often located at the frontotemporo-parietal convexity from bleeding of injured parasagittal or cortical veins
Equipment
- Mayfield head holder: clamp or horseshoe
- Basic craniotomy tray
- Burr hole tray
- High-speed drill with appropriate drill bits
- Bone flap fixation tray
- Hemostatic agents (Avitene, Gelfoam, Surgicel, bone wax)
- Intracranial pressure (ICP) monitor or external ventricular drain system if needed
Operating Room Set-up
- Headlight and loupes
- Bovie electrocautery
- Bipolar cautery
Anesthetic Issues
- Preoperative intravenous antibiotics administered within 30 min prior to incision (cefazolin 2 g intravenously or clindamycin 600 mg intravenously)
- Arterial line useful for blood pressure monitoring in acute SDH evacuation cases
- Load with phenytoin (15 to 18 mg/kg) administered slowly, or alternatively, levetiracetam 1000 to 1500 mg intravenously
- Communicate with anesthesiologist suspected degree of ICP elevation and if needed:
- Hyperventilation to pCO2 of 30 to 35 mm Hg
- Mannitol 0.5 to 1 g/kg infusion starting at time of skin incision
- Propofol (if indicated)
- Hyperventilation to pCO2 of 30 to 35 mm Hg
- Surgeon should warn anesthesiologist of potential hypotension at the time of clot evacuation as blood pressure is often supported by a sympathetic response to increased ICP
♦ Acute Subdural Hematoma
Intraoperative
Positioning
- In general, the patient should be semilateral with head neutral (since C-spine may not be cleared).
- Mayfield skull pin sites are kept out of the field and behind hairline and away from any skull fractures.
- Neck should be positioned to avoid compression of the jugular veins and kinking of the endotracheal tube.
- Ipsilateral shoulder elevation with a shoulder roll and head of bed elevation may be utilized to ensure good jugular venous outflow.
Planning of Incision
- Especially in emergency situations, ensure CT scan showing acute SDH is available in operating room where correct side can be verified.
- With electric clippers, a strip of hair of approximately ~3 cm in width is shaved over the planned incision or widely over the entire frontotemporoparietal area.
Incision and Scalp Flap
- Reverse question mark incision is begun 1 cm anterior to tragus, curved superiorly and posteriorly over the pinna, and extended to the midline and terminating at the hairline.
- Raney clips and bipolar cautery are used to control scalp bleeding.
- Temporalis muscle is divided in line with the incision and reflected anteriorly with the scalp flap.
Burr Holes
- Temporal burr hole placed first
- Additional burr holes placed as needed based on size/location of planned craniotomy
Craniotomy
- Use Penfield no. 3 to free the underlying dura from the bone.
- Craniotome is used to cut the craniotomy being sure to stay at least 1 to 2 cm lateral to midline to avoid the superior sagittal sinus.
- The bone flap is elevated with a periosteal dissector or Penfield no. 3.
- Either a cruciate opening or a U-shaped dural opening based anteriorly (Fig. 67.1), which is extended posteriorly as a T, can be utilized.
- Dural tenting sutures are placed circumferentially along the craniotomy edges.
Evacuation
- The hematoma is removed by using a combination of suction, forceps, and irrigation.
- Obtain hemostasis with bipolar cautery, Surgicel, Avitene, or Gelfoam.
- Inspect under the margins of the craniotomy to evacuate additional clot and to stop bleeding.
- Irrigate copiously to extract as much clot as possible.
Closure
- Close dura with 4–0 Nurolon sutures
- Place multiple central dural tack-up sutures and cover dura with Gelfoam or Duragen to minimize epidural space.
- Bone flap secured with titanium miniplates and screws
- If severe cerebral edema and refractory ICP elevation are anticipated, may consider insertion of ICP monitor or not replacing the bone flap
- Subgaleal drain is optional
- Temporalis muscle and fascial layers are closed with 0 or 3–0 Vicryl sutures
- Galea closed with inverted 3–0 Vicryl sutures
- Skin closed with staples
- Incision covered with Xeroform petroleum gauze dressing, 4 × 4 gauze, and a compressive head wrap
Postoperative
- Continue postoperative antibiotics for 24 hours
- Obtain postoperative head CT
- Patient is monitored in neurosurgery intensive care unit until stable
♦ Chronic Subdural Hematoma
Preoperative
Equipment
- Burr hole tray
- Horseshoe or Mayfield
Planning of Shave and Preparation
- Shave ~3 cm wide strip along planned incision
< div class='tao-gold-member'>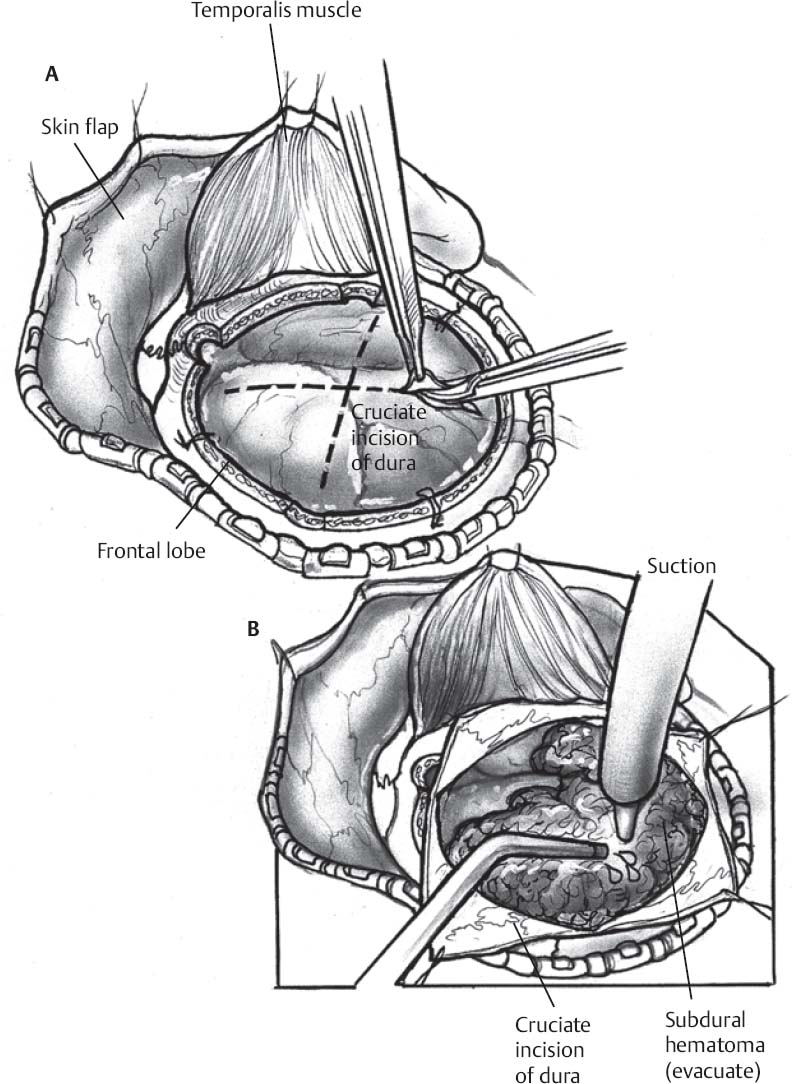 Only gold members can continue reading. Log In or Register to continue
Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


