♦ Preoperative
Operative Planning
- Patient counseling regarding surgical risks
- Magnetic resonance imagine (MRI)
- Computed tomography myelogram if MRI is inconclusive
- Flexion/extension x-rays if joint instability present
- Postoperative pain
- Potential joint instability
- Cranial nerve deficits
- Cerebrospinal f luid leak
- Posterior fossa syndrome (if intradural)
- Magnetic resonance imagine (MRI)
Equipment
- Basic tray
- Suboccipital tray
- High-speed drill (Midas Rex with M-35 and B-1 bits)
- Adson cerebellar retractors
- Intraoperative x-ray/fluoroscopy
Operating Room Set-up
- Headlight
- Loupes
- Microscope (optional)
- Bipolar and Bovie cautery
- Intraoperative x-ray
- Mayfield head holder
- Assess patient’s pulmonary function for ability to tolerate prone position
- Prophylactic intravenous antibiotics (cefazolin 2 g for adults) 30 minutes prior to incision. Consider vancomycin if instrumentation is planned.
- Foley catheter for prolonged surgery
- Consider electrophysiologic monitoring (e.g., somatosensory evoked potentials)
♦ Intraoperative
Positioning
- Prone position with appropriate padding to prevent pressure neuropathies
- Arms tucked at sides
- Mayfield head holder or tongs with traction to secure head in capital flexion
- Mild reverse Trendelenburg position to improve venous drainage
- Mayo stand above head
Planning of Minimal Shave
- Use disposable clippers
Planning of Sterile Scrub
- Betadine detergent scrub with sterile gloves
- Sterile towel to dry
- Incision is marked
Exposure
- Midline skin incision from the inion to the second or third cervical vertebrae
- Subperiosteal dissection continued in the midline until the occiput and spinous processes of C2 are exposed
- Foramen magnum and C1 cleared of muscular attachments using periosteal elevators and curettes
- Bipolar cauterization to control bleeding from paravertebral venous complex
- Self retaining retractor is placed
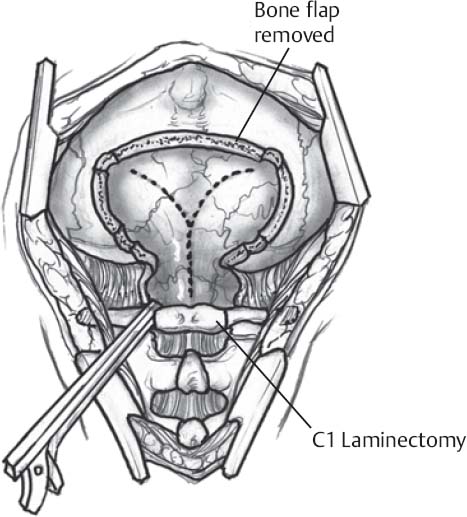
♦ Suboccipital Bone Removal (Fig. 90.1)
- Not required significantly for typical occipitocervical fusion
- Craniotomy
- Suboccipital area inferior to inion decompressed by removal of posterior lip of foramen magnum using high speed drill and or Kerrison rongeurs with thin footplate
- B-1 with footplate and Kerrison rongeur used to perform craniotomy from lateral edge of the foramen magnum (alternatively can perform craniec-tomy with drill/rongeurs)
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel
- Suboccipital area inferior to inion decompressed by removal of posterior lip of foramen magnum using high speed drill and or Kerrison rongeurs with thin footplate





Full access? Get Clinical Tree


