Chapter 20 Surgical Techniques for Nerve Tumors
Benign Tumors
Incision
• The surgical approach is tailored according to the nerve and the level involved, but the major principles are similar. When possible, the nerve leading into and out of the tumor should be exposed.
• This usually requires a longitudinal incision on the limb, neck, or shoulder and not a short or transverse incision.
• Excellent exposure of structures adjacent to and both proximal and distal to the lesion is paramount. Adjacent nerves, vessels, or other adherent structures must also be dissected away and protected.
Dissection of Fascicles Around the Tumor
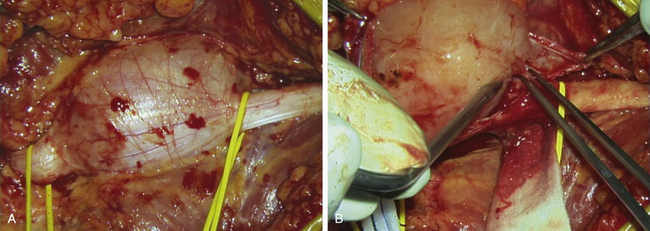
• The majority of these lesions, whether schwannoma or neurofibroma, are intraneural in locus. The tumor has usually displaced, thinned out, and “basketed” the fascicles so that they encircle the lesion (Figure 20-1). Sometimes the neural sheath tumor has grown in an eccentric fashion, displacing most fascicles to one side of the mass (Figure 20-2).
• It is usual to begin by making a longitudinal incision between the fascicles that are spanned or basketed around the tumor.
• The best spot for this is usually on the circumference of the tumor, where the fascicles are not so closely compacted.
• The pseudocapsule, if present, is opened, and this and the fascicles are gradually worked away from the tumor itself (Figure 20-3).
• This intraneural dissection can be done with a variety of tools. The perineurium of fascicles is preserved. Accuracy is essential and is most easily achieved by microsurgical technique with magnification. The patient should not incur any additional neurological deficit unless the case is especially complex.
• Fascicles are gradually moved to either side and away from the tumor mass.
• Because there is usually fascicular input and output to the tumor itself, an interfascicular dissection of the nerve is done at both the proximal and distal poles of the tumor.
• In this way, most fascicles can be traced into the base and sides of the capsule, and the specific fascicles that enter and leave the neoplasm can be identified (Figure 20-4).
• If the tumor is a schwannoma, the intraneural fascicle is usually a single, fairly small fascicle at either end entering and leaving the core of the tumor.
• Nerve stimulation of such a fascicle usually gives a negative response. This means that the entering and leaving fascicle can be sectioned without functional loss.
• This fascicle is usually isolated by a plastic loop, evaluated, and then sectioned proximal and distal to the tumor. The tumor is then removed as a solitary mass.
• If the entering and leaving fascicles are examined histologically, one sees a rudimentary array of immature, poorly developed axons. These fibers are small and poorly myelinated, and the surrounding structure is disorganized.
• In the case of neurofibromas, there may be more than one fascicle entering and leaving the substance of the tumor; if there is a single fascicle, it is usually larger than those seen in schwannomas.
• It is very important to work out the fascicular anatomy at both the proximal and distal poles of such lesions.
• What appear to be fascicles intrinsic to the neurofibroma are often shown to be external to the bulk of the tumor when the polar anatomy is displayed.
• The entering or leaving fascicles are sectioned and used as a handle. The tumor is then elevated out of and away from its fascicular structure until the opposite pole is reached; the residual entering or leaving fascicles are then sectioned, and the tumor is totally removed.
• The distinction between a solitary schwannoma and a neurofibroma may be obvious at surgery, or the distinction may only be apparent at pathological examination of the specimen.
• The risk of causing neurological loss by careful excision of a schwannoma is very small, but that statement does not apply to neurofibroma cases. Functioning fascicles may be intrinsically enmeshed within the tumor, so that stimulation and, if necessary, NAP studies must be conducted with care. Significant clinical judgment is required in making the decision to cut functioning fascicles, which may be needed to totally excise a tumor.
• The informed consent and good clinical judgment may lead the surgeon to a subtotal excision or to retreat after a biopsy without any definitive surgery. These cases are followed with intermittent clinical examination and scans.
• Neither overly timid nor overly aggressive surgery serves the patient well. A skilled, experienced microsurgeon will be able to weigh the risks and excise a focal neurofibroma with relative safety. Such a surgeon knows when to quit when local conditions indicate that the stakes are becoming too high.
• There are no small or easy operations. Surgeons embarking on a simple schwannoma excision may occasionally find that they are confronted with a difficult neurofibroma. Mismanaging such a case will have unfortunate consequences for the patient and possible unfortunate medicolegal consequences for the surgeon.
< div class='tao-gold-member'>






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


