(Reproduced, with permission, from Hauser SL. Harrison’s Neurology in Clinical Medicine. 2nd ed. New York: McGraw-Hill; 2010:191.)
a. Area 8 of frontal cortex
b. Cranial nerve III
c. Cranial nerve VI
d. Medial longitudinal fasciculus
e. Pontine paramedian reticular formation
345. A patient is seen by a neurologist because he had problems of ambulation and vision. Specifically, the patient presents with the following signs and symptoms: spasticity, visual blurring, ataxia, paresthesias (such as tingling sensation and painful burning), diplopia, and bladder dysfunction. The MRI shown here demonstrates a number of abnormalities as shown by the arrows. This patient suffers from which of the following disorders?
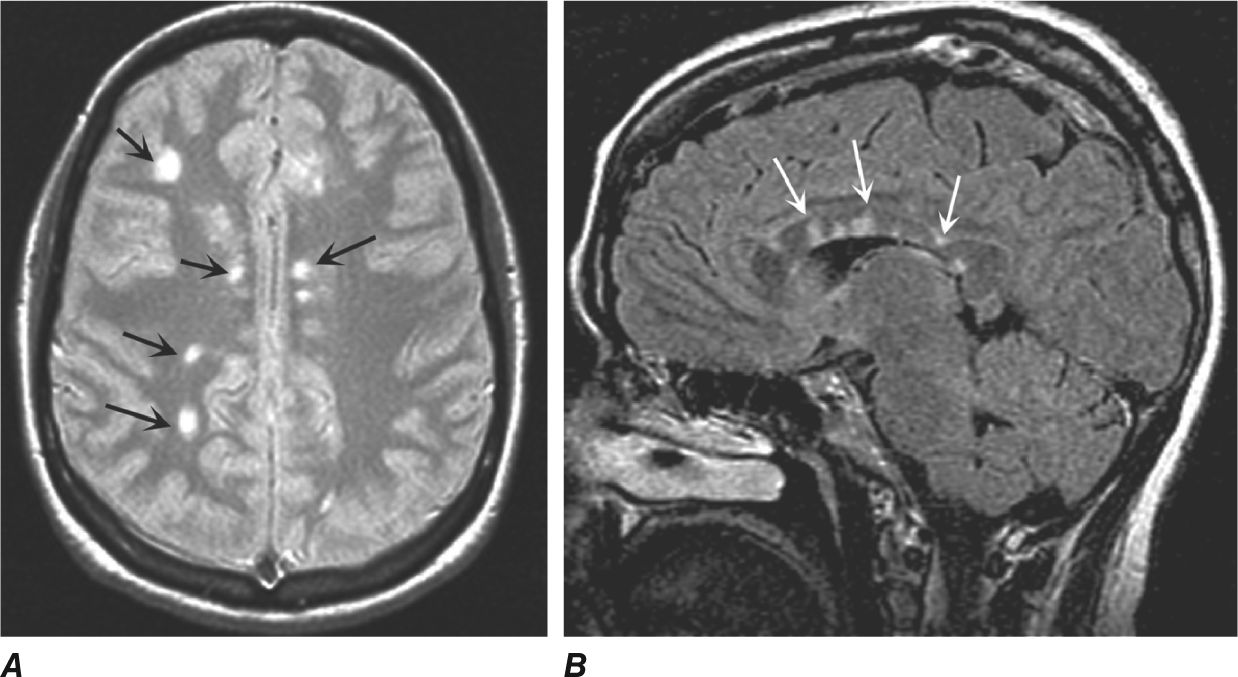
(Reproduced, with permission, from Hauser SL. Harrison’s Neurology in Clinical Medicine. 2nd ed. New York: McGraw-Hill; 2010:441.)
a. Stroke
b. Encephalitis
c. Brain abscess
d. Multiple sclerosis
e. Bacterial meningitis
346. Sensory testing is administered to a 65-year-old man because he is unable to make sensory discriminations as well as to integrate temporal and spatial sensory information. Moreover, his ability to recognize position sense is disturbed, although other modalities, including touch, pain, vibration, and temperature sensations, are preserved. On the basis of these observations, where is the most likely site of a lesion that could account for this form of deficit largely limited to position sense?
a. Dorsal root ganglia
b. Substantia gelatinosa
c. Dorsal columns
d. Dorsal column nuclei
e. Parietal cortex
347. A patient who had been suffering from a very serious and prolonged bout with viral encephalitis goes to see his internist as he begins to recover and complains that he has lost his ability to identify the taste of different foods. Which of the following is the most likely explanation for the loss of taste sensation?
a. Damage to the geniculate ganglion
b. Inflammation of the chorda tympani
c. Degeneration of solitary nucleus neurons
d. Pathological changes in taste buds
e. Inflammation of the lingual nerve
348. A patient complains about partial loss of vision in his left eye. After a thorough examination, it is determined that he has an island of impaired vision surrounded by normal vision (ie, scotoma). Further examination, including an MRI, determined that the defect was associated with a lesion in which of the following regions?
a. Optic nerve
b. Optic tract
c. Lateral geniculate nucleus
d. Geniculo-calcarine tract
e. Area 17 of the right visual cortex
349. A patient has had a congenital disorder for many years involving his visual system. At one point, the patient was referred to a Neuro-ophthalmologist who identified the disorder achromatopsia, where the patient is unable to see colors and his visual acuity is reduced. In this case, the patient suffers from a left hemiachromatopsia. All other visual functions appear normal. A subsequent MRI identifies a lesion in the brain. Where would the neuro-ophthalmologist expect to see this lesion?
a. Superior aspect of area 17 of right visual cortex
b. Right lateral geniculate nucleus
c. Right optic tract
d. Right inferotemporal region
e. Right middle temporal cortex
350. A 75-year-old man goes to his ophthalmologist after he experiences difficulty in seeing out of his left eye. In that eye, his visual acuity is limited to the perception of light only, while his vision in his right eye is normal (ie, 20/20). The ophthalmologist concludes that a lesion causing this deficit is situated in which of the following regions?
a. Left optic nerve
b. Optic chiasm
c. Left optic tract
d. Left lateral geniculate nucleus
e. Left occipital cortex
351. Following a viral infection, a patient complains about difficulty in being able to detect tones. An audiology examination further confirms this deficit indicating that the patient is unable to discriminate among different tones. Which of the structures if damaged by the viral infection would account for the loss of his ability to discriminate tones?
a. Basilar membrane
b. Tympanic membrane
c. Otolithic membrane
d. Superior olivary nucleus
e. Middle temporal gyrus
352. A 74-year-old woman is referred to a neuro-ophthalmologist after her internist observed that she has a visual deficit. It is noted that her pupils are not of the same size. In addition, when light is shone in the right eye there is constriction of the left pupil. However, there is no movement (ie, constriction) of the pupil of the left eye. The neuro-ophthalmologist concludes that the patient has a lesion of which of the following regions?
a. Right optic nerve
b. Right lateral geniculate nucleus
c. Left primary visual cortex
d. Right oculomotor nerve
e. Right retina
353. An elderly man is taken to the emergency room after he complains that he has difficulty seeing out of his left eye. In addition, there is a reduction in his vision in the left hemi-field of each eye. The patient appears to show no other signs or symptoms other than the failure to see out of one eye. A neurological test is conducted, which included an MRI, and it is concluded that he had a small stroke. In which of the following arteries could there have been an occlusion that could account for this deficit?
a. Right superior cerebellar artery
b. Right middle cerebral artery
c. Right posterior cerebral artery
d. Right ophthalmic artery
e. Circle of Willis
354. A patient is seen by a neuro-ophthalmologist after having complained about problems in seeing. Specifically, this patient is unable to look upward and also shows a loss of accommodation, convergence nystagmus, and ptosis. An MRI reveals a brain lesion. In which of the following structures could such a lesion account for the deficits observed in this patient?
a. Oculomotor nerve (III)
b. Trochlear nerve (IV)
c. Abducens nerve (VI)
d. Pontine gaze center
e. Posterior commissure
355. A patient complains to his ophthalmologist that he has difficulty in following moving objects, which is especially noted when he is watching cars on the highway. He later has an MRI which detects that the patient has indeed suffered a stroke. Which of the following arteries is affected in this case?
a. Posterior cerebral artery
b. Superior cerebellar artery
c. Anterior cerebral artery
d. Middle cerebral artery
e. Lenticulostriate artery
356. A 74-year-old man has a brain hemorrhage shown in the MRI below. On the basis of the locus of the lesion, which of the following would best describe the deficits incurred by the patient?
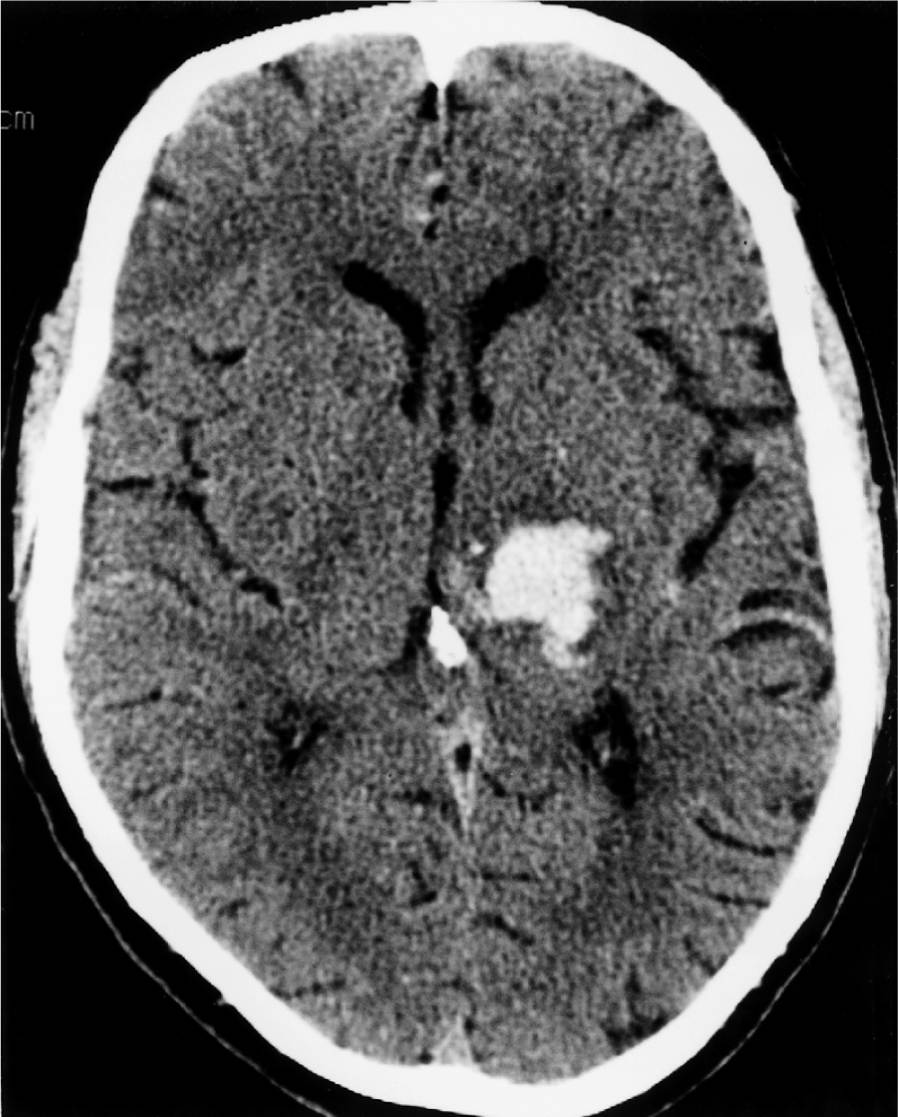
CT scan of a left thalamic hemorrhage that caused hemiplegia and hemisensory loss in a hypertensive patient. A small amount of blood is seen in the adjacent posterior third ventricle. (Reproduced, with permission, from Ropper AH. Adams & Victor’s Principles of Neurology. 9th ed. New York: McGraw-Hill; 2009. Fig 34-21.)
a. Finger agnosia
b. Apraxia
c. Sensory neglect
d. Hemi-somatosensory loss
e. Dyskinesia
Sensory Systems
Answers
313. The answer is e. (Ropper, pp 211, 950. Purves, p 265.) In one form of retinitis pigmentosa, there is a genetic defect with respect to rhodopsin. The result of this defect is the production of defective opsin. As a consequence, rod cells are affected, leading to a reduced response to light. Consequently, there is degeneration of photoreceptors which die by apoptosis. At a later time, cone cells also appear to degenerate. Other components of the retina (such as retina/ganglion cells) and CNS neurons (such as those located in area 17) are not directly affected and vision is not totally lost.
314. The answer is d. (Kandel, pp 512-521. Siegel and Sapru, pp 275-281.) The only cell in the retina that is capable of producing an action potential is the ganglion cell. As indicated earlier, the ganglion cell gives rise to optic nerve fibers, which terminate as optic tract fibers in the lateral geniculate nucleus. As a result of action potentials generated in the ganglion cells, volleys of impulses are transmitted over these fibers, resulting in the appropriate responses in the neurons of the lateral geniculate nucleus. Therefore, the patient became blind of damage to the ganglion cells whose axons form the optic nerve and optic tract, thus depriving the lateral geniculate nucleus and visual cortex from receiving visual inputs.
315. The answer is c. (Purves, pp 254-257. Siegel and Sapru, pp 286-287.) To correct for farsightedness, a person is prescribed a convex lens because objects focus behind the retina. The convex lens helps to refocus the object onto the retina. The reason that the focus of the object is behind the retina is because the eyeball is too short.
316. The answer is b. (Aminoff, pp 131-138, 144-147.) Calcification of the internal carotid artery could serve to disrupt nerve fibers proximal to it. One such group of fibers includes parts of the optic nerve. In this case, the component of the affected right optic nerve includes the lateral aspect, or those fibers that mediate vision associated with the nasal visual field of the right eye. If the damage were more extensive and if it involved the entire nerve, then total blindness of the right eye would have occurred.
317. The answer is b. (Siegel and Sapru, p 289. Aminoff, pp 131-138, 144-147.) A tumor pressing on the optic chiasm will disrupt the optic nerve (and tract) fibers that cross to the opposite side. These fibers mediate vision associated with fibers arising from the nasal retina of each eye. Since the nasal retina of each eye is associated with the temporal visual field for each eye, the visual loss is referred to as a bitemporal hemianopsia.
318. The answer is c. (Siegel and Sapru, p 289. Aminoff, pp 131-138, 144-147.) Disruption of optic tract fibers destined for the lateral geniculate nucleus will cause a homonymous hemianopsia because it affects fibers arising from the temporal retina of the ipsilateral side and from the nasal retina of the contralateral side. Since the damage occurred in the left optic tract, the loss of vision is reflected on the right visual field (ie, the left temporal retina is associated with the nasal [or right] visual field of the left eye, and the right nasal retina is associated with the temporal [or right] visual field of the right eye). Therefore, such a lesion would result in a right homonymous hemianopsia.
319. The answer is d. (Siegel and Sapru, pp 289-290. Aminoff, pp 131-138, 144-147.) From the lateral geniculate nucleus, there are two trajectories that the fiber pathways take en route to the visual cortex. One pathway passes dorsally through the parietal lobe and terminates in the upper bank of the calcarine fissure in the ipsilateral primary visual cortex. The second pathway takes a more circuitous (ventral) route—called the Meyer-Archambault loop—through the temporal lobe and terminates in the lower bank of the calcarine fissure in the ipsilateral primary visual cortex. The lower bank of the calcarine fissure is associated with the upper visual quadrants of the contralateral visual fields for both eyes, while the upper bank of the calcarine fissure is associated with the lower quadrants of the contralateral visual fields for both eyes. Thus, if there is a lesion of the left temporal lobe affecting the Meyer-Archambault loop, then the right upper quadrant for each eye will be affected. This deficit is referred to as a right upper quadrantanopia.
320. The answer is e. (Siegel and Sapru, pp 289-290. Aminoff, pp 131-138, 144-147.) The reasoning underlying the answer to this question is exactly as presented in the explanation of the answer to Question 334. In brief, fibers from the left lateral geniculate destined for the upper bank of the calcarine fissure will mediate visual impulses associated with lower quadrants of the right visual fields for both eyes. This deficit is referred to as a right lower quadrantanopia.
321. The answer is d. (Kandel, pp 433-440, 451-457
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


