The Electrical Brain
MORE THAN CHEMISTRY
One of our favorite illustrations in this book is Figure 3.9, which highlights the electrochemical configuration of neural communication. Unfortunately, many mental health professionals view psychiatric disorders as exclusively chemical in nature. The term “chemical imbalance” is part of our cultural lexicon, a perspective that misses the rapid signals passed over long distances before any chemicals are released.
Electricity is the currency of the brain. It is not just chemistry—the brain is an electrical organ. This is not new information, but rather a different, newer, and more nuanced way to view the brain. The brain uses enough electricity to power the 20 W light in your refrigerator—if it was possible to harness the electricity in your brain. That is a significant amount of electrical energy! Merely keeping our brains running requires about 20% of all the calories we consume, and higher amounts when we concentrate (as opposed to watching TV).
We believe the electrical side of the electrochemical signal has been ignored for too long. This chapter—new to the second edition—has been added to correct the inequity. Probably the real impetus is not so much an attempt to be fair, but our reaction to the explosion of research on the effects of electrical manipulation of the brain.
History of Electrical Stimulation
Before it was possible to produce electricity on demand, the ancient Greeks and Romans reportedly used fish—electric eels or rays—to stimulate the brain as a treatment for intractable headaches. Of course the ancient physicians did not know they were using electricity and the clinical effectiveness of electrical eels for headaches is unknown. However, it is relevant to note that eNeuras Therapeutics is seeking the Food and Drug Administration (FDA) approval for a handheld device that delivers a brief electromagnetic pulse (transcranial magnetic stimulation—more on this later) to the back of the head to “short circuit” an impending migraine. So, maybe an electric ray could actually have stopped an ancient headache. (If someone tries out the eel headache therapy, please write us and let us know of the outcome. [We certainly aren’t recommending that you try this.])
In the first chapter we mentioned Luigi Galvani who in 18th century Italy demonstrated that electrical sparks could induce movement in an amputated frog’s leg. He was the first to propose that the brain generates intrinsic electricity that spreads down through the nerves to the muscles. He believed electricity was the mysterious “vital force” controlling the body. His nephew Giovanni Aldini (1762-1834) spent many years conducting further research and promoting the beliefs of his uncle. Using primitive batteries developed by Volta, Aldini applied electrical stimulation to mammals and eventually even humans. He demonstrated throughout Europe—part science, part carnival—the effects of applying electrical stimulation to human cadavers. In London in 1803 at the Royal College of Surgeons, Aldini applied electrical stimulation to a freshly hung criminal and awed his audience with facial and body movements in the deceased human. Aldini’s work was an inspiration for Mary Shelley’s novel Frankenstein.
Of even greater interest were Aldini’s efforts to treat the mentally ill with electrical stimulation. He is reported to have treated an Italian farmer suffering from melancholy madness with stimulation applied to the patient’s shaved, damp head (Figure 10.1). After several weeks of treatment, the patient was well enough to return to his family. Later, Aldini met the famous French psychiatrist Philippe Pinel—the man who removed the chains from the insane—and applied his “galvanic” treatment to several patients at La Salpêtrière Hospital,
but with limited success. We do not fully understand the doses and actual current that Aldini used, but today a different version of this type of treatment is called transcranial direct current stimulation (tDCS). While not FDA approved or even in regular use, tDCS is being studied as a possible intervention for Parkinson’s disease, tinnitus, post-stroke deficits, and, you guessed it, just like Aldini demonstrated, melancholy (depression). tDCS involves passing a small (2 mA) direct current through the brain for 20 to 30 minutes. The brain regions under the anode become excited, and it takes less energy for that region to carry out its normal function.
but with limited success. We do not fully understand the doses and actual current that Aldini used, but today a different version of this type of treatment is called transcranial direct current stimulation (tDCS). While not FDA approved or even in regular use, tDCS is being studied as a possible intervention for Parkinson’s disease, tinnitus, post-stroke deficits, and, you guessed it, just like Aldini demonstrated, melancholy (depression). tDCS involves passing a small (2 mA) direct current through the brain for 20 to 30 minutes. The brain regions under the anode become excited, and it takes less energy for that region to carry out its normal function.
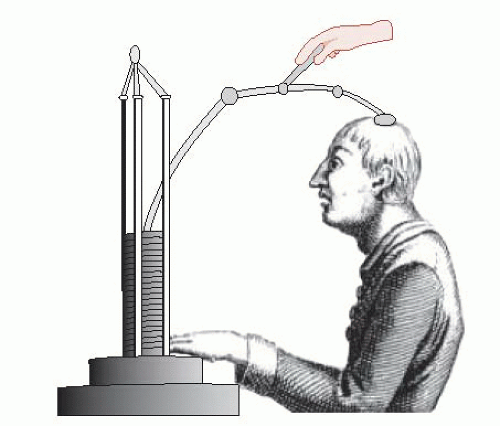 FIGURE 10.1 • A patient receiving a crude form of direct current brain stimulation in 1803. As the brain is an electrochemical organ, it can be changed and manipulated with externally applied electricity. (Adapted from Parent A. Giovanni Aldini: from animal electricity to human brain stimulation. Can J Neurol Sci. 2004;31(4):576-584.) |
Wilder Penfield is another one of the great figures that pioneered the use of electricity to study the brain. Penfield crossed paths with some of the leading neuroscientists mentioned in the first chapter. As a Rhodes scholar, he studied in Sherrington’s lab at Oxford and later collaborated with Ramóny Cajal in Madrid. However, Penfield was a practicing neurosurgeon in Canada who studied the brain while he was treating patients. He perfected what came to be called the Montreal Procedure: the surgical removal of the site of the brain causing intractable seizures—still the most effective treatment for disabling epilepsy.
The unique aspect of the Montreal Procedure was the exploration of the patient’s brain while they remained awake. Using local anesthesia, the patient’s skull was opened and their brains exposed. Penfield gently stimulated the cortex around the lesion with an electrode. Patients remained alert so they could identify what they felt or moved as Penfield applied the electricity. The goal was to identify the pathological tissue, but preserve as much of the healthy brain as possible. (Interested readers can see reenactments on YouTube by searching for “Wilder Penfield.”)
While Penfield was treating these patients, he was also mapping out the sensory and motor cortex. For each patient he would record the location where different body parts were represented on the cortex. For example, Figure 10.2A shows the location of facial and eye sensations and movements for a number of patients. Figure 10.2B shows average location for the motor cortex compiled from data on almost 400 patients over 20 years. We now know the sensory and motor homunculus are not static, but are capable of reorganization after injury or with frequent use as we discussed in Chapter 8.
Penfield is best known in popular culture for awakening memories with electrical stimulation of the temporal lobes. This has led to the perception that memories are a fixed neural network (or engram) that can be repeatedly elicited when stimulated. The reality is not so impressive. It turns out that only about 8% of people whose temporal lobes were stimulated reported any memory. Of those that did “remember,” most reported experiences similar to the aura that preceded their seizure or described something more like a hallucination. Furthermore, modern studies have failed to find clear memories that reproduce with each stimulation. A memory engram remains elusive.
In the late 1930s, around the time Penfield was refining the Montreal Procedure, Ugo Cerletti, an Italian physician, began using electricity to induce seizures as treatment for the seriously mentally ill. Although this may seem like an extreme intervention to us, it was actually a logical step in the progression of physical treatments of mental illness. Psychiatrists had been inducing convulsions with metrazol—a γ-aminobutyric acid (GABA) antagonist that increases neural excitability, but it was difficult to control. Cerletti saw an electrically induced seizure as a cleaner procedure: easier to induce and terminate—no residual metabolite to complicate the recovery. Cerletti’s intervention has developed into electroconvulsive therapy (ECT) and remains the most effective treatment for depression.
The last historical figure we choose to discuss is Robert Heath, a psychiatrist and neurologist who in the late 1950s coordinated the placement of electrodes into the brains of patients with serious mental illness. He was influenced by the work of Olds and Milner (see Figure 12.2) and was hoping that small frequent doses of electricity applied directly
to deep sectors of the brain might improve their mental condition. He conceptualized his intervention as an emotional pacemaker. (Interested readers can view actual clips of one patient by searching “Robert Heath” on YouTube.) The results were disappointing and his approach was controversial. However, Heath’s work was the forerunner of deep brain stimulation (DBS), now a common intervention for Parkinson’s disease—and something of great interest to many as a possible treatment for intractable depression.
to deep sectors of the brain might improve their mental condition. He conceptualized his intervention as an emotional pacemaker. (Interested readers can view actual clips of one patient by searching “Robert Heath” on YouTube.) The results were disappointing and his approach was controversial. However, Heath’s work was the forerunner of deep brain stimulation (DBS), now a common intervention for Parkinson’s disease—and something of great interest to many as a possible treatment for intractable depression.
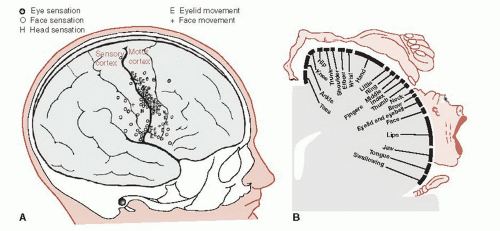 FIGURE 10.2 • Actual recordings of sensation and movement for the eyes and face of patients examined by Wilder Penfield (A) compared with the cumulative motor homunculus for the average patient (B). (Adapted from Penfield W, Boldrey E. Somatic motor and sensory representation in the cerebral cortex of man as studied by electrical stimulation. Brain. 1938;60:389-443.) |
BIOELECTRICITY
All living cells maintain a negative electrical charge. That is, they are more negative inside relative to the extracellular space. Nerve cells utilize this property to communicate with one another— a process that through millions of years of evolution has transformed the speed by which biological organisms sense and respond. Without bioelectricity, we would all be slower than slugs.
The negative charge inside a cell is the product of competing forces within the cellular realm. First and foremost, the cellular wall creates a boundary that limits the movement of charged substances into or out of the cell. The primary negative charge created in a cell is contained on the negatively charged organic molecules within the cell, for example, amino acids. These large molecules, too large to escape through the cell wall, provide the bulk of the negative charge inside the cell.
The negative charge inside the cell is reduced by the movement of positive ions, such as potassium (K+) and sodium (Na+), into the cell. The positive ions are attracted to the negative charge inside the cell: remember, opposites attract in love and electricity. However, the movement of each ion is different. The K+ ions flow freely into the cell until they reach a point at which the forces of the concentration gradient start to pull some K+ back into the extracellular space. The propensity of ions to evenly diffuse within a contained space is called the concentration gradient. Ultimately, the amount of K+ inside the cell is a product of the pull of the electrostatic forces into the cell and the push of the concentration gradient back out to the extracellular space.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


