The Internal Carotid Artery
Key Points
The extracranial and ophthalmic branches of the internal carotid artery exist in a state of actual or potential exchange with distal branches of the external carotid artery. During endovascular interventions one must be ever attentive to the possibility of inadvertent reflux of embolic material in the wrong direction through these routes. The greatest of these risks is with the ophthalmic artery.
Minor or rare variants of the branches of the internal carotid artery are important to recognize in every patient so that catastrophic surgical and endovascular calamities can be avoided.
The common carotid artery usually bifurcates at the C3–C4 level into an external carotid artery trunk and an internal carotid artery. The bifurcation may be lower, occasionally being seen as low as T2–T3, although such extremes are rare (Fig. 10-1) (1). Most carotid angiograms are performed on older patients in whom the possibility of atherosclerotic change demands an evaluation of the bifurcation before catheterization of the internal carotid artery (Fig. 10-2). There are other situations in which it is prudent or imperative to perform an angiogram of the common carotid bifurcation before further catheterization or wire manipulation. Some of these are obvious and include questions related to the cervical internal carotid artery itself, for example, dissection, pseudoaneurysm, tumor involvement, and the like (Figs. 10-3–10-6). Others are less obvious but encompass any situation in which the final interpretation of the angiogram might be seriously compromised by the presence of a minimal amount of cervical carotid spasm induced by the wire, for example, evaluation of subtle tumor encasement or traumatic injury (Figs. 10-7–10-9).
Anatomy of the Internal Carotid Artery
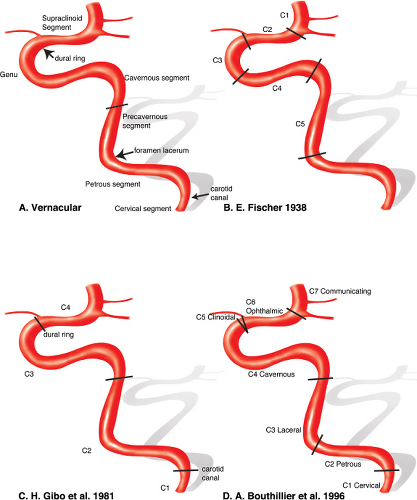
The anatomy of the internal carotid artery is described in segments between the common carotid bifurcation in the neck and the supraclinoidal internal carotid bifurcation. In ascending order, these consist broadly of the cervical, petrous, precavernous, cavernous, paraclinoidal, and supraclinoidal segments (Fig. 10-10).
Cervical Segment
This segment spans the common carotid bifurcation to the skull base. At the base of the skull, the internal carotid artery lies anteromedial to the internal jugular vein with which it shares a neurovascular sheath. This sheath also encloses the IX, X, XI, and XII cranial nerves and postganglionic sympathetic fibers. The pharyngeal wall lies directly anteromedial to the carotid artery. Instrumentation or biopsy of the Rosenmuller fossa carries a risk of internal carotid injury. Such injuries are also more likely in the setting of unsuspected pharyngeal loops of the internal carotid artery, particularly where these loops have a more medial or directly submucosal course (sometimes confusingly referred to as an aberrant carotid artery, not to be confused with the more important variant by the same name taking a route through the middle ear). Parapharyngeal infections may involve the wall of the carotid artery at this level with a risk of pseudoaneurysm formation. At the exocranial ostium of the carotid canal, the carotid sheath splits into two layers. The inner layer becomes the periosteum of the carotid canal; the outer becomes the exocranial periosteum. The cervical segment usually does not have any branches (Fig. 10-11).
Petrous Segment and Laceral Segment
The petrous segment of the internal carotid artery consists of a vertical and a horizontal portion (Fig. 10-12). It enters the skull base at the exocranial opening of the carotid canal, ascends approximately 1 cm, and then turns anteromedially until it enters the intracranial space at the foramen lacerum. The laceral segment is a continuation of the petrous segment ending at the petrolingual ligament (2,3). The artery is accompanied along its course by the sympathetic fibers of the stellate ganglion and by a venous plexus (4,5). Some of the sympathetic fibers part company from the internal carotid artery at the foramen lacerum and form the deep petrosal nerve. The deep petrosal nerve joins the parasympathetic fibers of the greater superficial petrosal nerve to become the Vidian nerve. This nerve travels anteriorly to the pterygopalatine fossa via the Vidian (pterygoid) canal. Angiographically, branches of the petrous internal carotid artery are uncommon, but at least three possible branches are worth remembering: The caroticotympanic branch, the mandibulovidian branch, and the variant stapedial artery.
 Figure 10-1. Unusually low bifurcation of the left common carotid artery close to the thoracic inlet. Such anomalies are rare. Variants such as this can be confusing when the catheter is advanced obliviously into the distal external carotid artery without the benefit of an aortic arch injection ahead of time. One can then be deceived into thinking that the vessel injected is the sequelae of an internal carotid artery occlusion or agenesis, unless one retracts the catheter very proximally to find the bifurcation. |
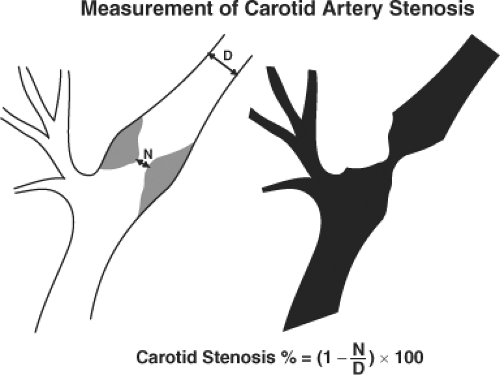 Figure 10-2. Measurement of carotid artery stenosis. The formula for calculation of the percentage stenosis of the internal carotid artery is illustrated according to the North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria. In situations of advanced stenosis, the distal diameter of “normal” vessel, (D), is attenuated or underopacified, leading to an underestimation of the percentage stenosis. (Label: N, diameter of stenosis segment at the most severe point.) |
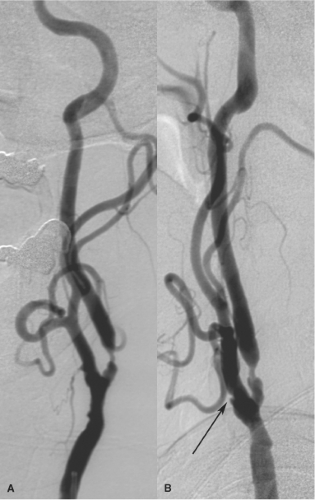 Figure 10-3. (A–B) Recurrent left internal carotid artery stenosis following previous endarterectomy. This 81-year-old patient was referred for left carotid angioplasty and stenting with asymptomatic recurrent disease 2 years after a previous endarterectomy with Doppler estimates of 90% stenosis. The hints that this is a previously operated-on artery include the extension of irregularity into the external carotid artery with a “cuff” or shelflike appearance (arrow in B). As is frequently the case, the final calculation of the degree of stenosis depends very much on where one places the calipers, but the calculation should always be done on the view showing the degree of stenosis at its most severe—in this instance, the AP view (A). |
 Figure 10-4. (A–B) String sign of preocclusive carotid disease. In this patient, the internal carotid artery opacification (arrowheads) happens later than expected in the film sequence due to the advanced degree of stenosis with contraction of the lumen of the artery. (Labels: A, AP view, B, lateral view.) When a string sign such as is seen here is demonstrated, it can be very important to verify that the flow is antegrade in the internal carotid artery (indicating the viability of the still patent vessel) and that the occluded artery is not filling retrogradely from above, through cavernous or ophthalmic collaterals. |
 Figure 10-5. Carotid ulceration. A factor not taken into account by a simple calculation of the degree of stenosis of a carotid artery is the quality or thrombogenic potential of the substrate of the stenosis. In this case, the degree of stenosis as measured by NASCET criteria would be approximately 50% to 60%. However, the prominent ulcer (arrow) suggests that this is a more troublesome lesion than a smooth, inactive 50% stenosis in another patient. Presumably, the ulcerated appearance is the remnant of a prior plaque rupture, followed by excavation and pitting of the plaque site. |
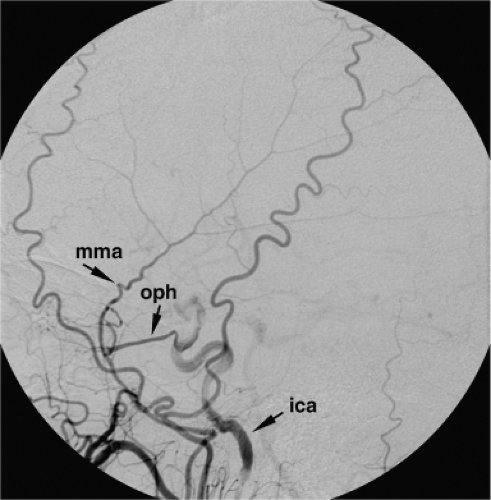 Figure 10-6. Complete occlusion of the carotid artery with retrograde flow to the petrous segment. In this patient, the internal carotid artery (ica) is already occluded. The external carotid artery fills the middle meningeal artery (mma), which gives a big collateral branch to the ophthalmic artery (oph). The ophthalmic artery flows retrogradely to the internal carotid artery, where there is antegrade and retrograde opacification of the carotid vessel. Note the density change as the ophthalmic artery enters the carotid artery due to dilution. |
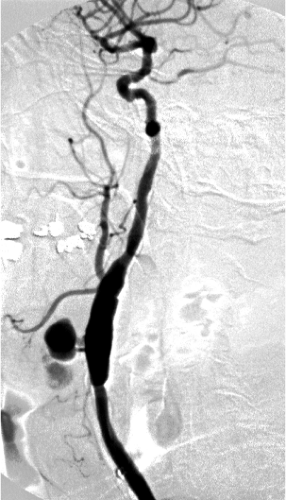 Figure 10-7. Anastomotic breakdown in a left carotid graft. A jet of contrast directed anteriorly fills a multilobulated pseudoaneurysm, which presented as a pulsatile mass. |
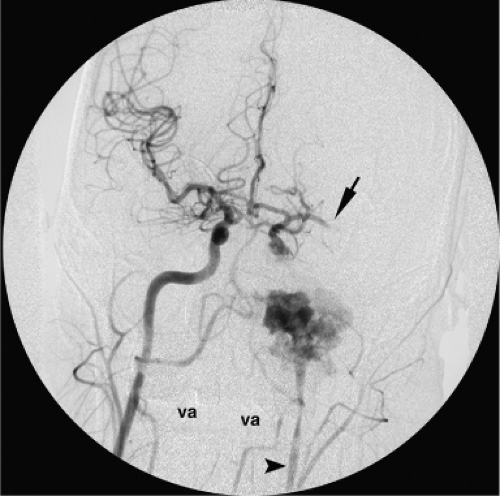 Figure 10-8. Laceration of the internal carotid artery. Frontal view of the head during an arch aortogram showing a complete transection of the left internal carotid artery and absence of flow in the left middle cerebral artery (arrow). There is reflex spasm or collapse of the walls of the left internal carotid artery (arrowhead). va, vertebral artery. |
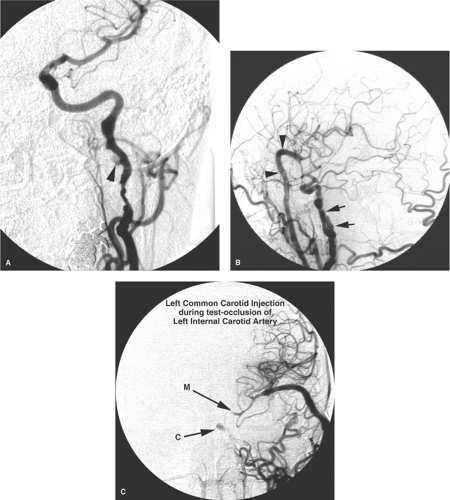 Figure 10-9. (A–C) Dissecting pseudoaneurysms of the internal carotid artery. A: A middle-aged female with angiographic and clinical evidence of deterioration in a left internal carotid artery dissection, even with adequate anticoagulation. A left common carotid artery injection demonstrates irregular attenuation of the artery with pseudoaneurysm or pouch formation at the skull base (arrowhead). Significant other observations on this image include the absence of collateral flow through the circle of Willis. The marginal degree of collateral flow was confirmed on injections of the other cerebral vessels. The patient was advised to undergo a bypass procedure to the left hemisphere, to be followed by endovascular occlusion of the left internal carotid artery. B: A left common carotid artery injection, lateral projection, after a venous graft bypass (arrowheads) from the left external carotid artery to the left middle cerebral artery. The complex architecture of the pseudoaneurysms can be seen on this oblique projection (arrows). C: A frontal projection of a left common carotid artery injection made proximal to an occluding test balloon placed proximally in the left internal carotid artery. Reconstitution of the left cavernous internal carotid artery (C) via collaterals from the external carotid artery is seen. The M1 segment of the left middle cerebral artery (M) opacifies retrogradely from the anastomotic site. |
 |
Caroticotympanic Branch of the Petrous Internal Carotid Artery
This branch of the petrous internal carotid artery is usually too small to see or is obscured by dense petrous bone. It is a vestige of the course of the hyoid artery. Apart from its role as a vestigial remnant in understanding vascular anomalies of the middle ear, the importance of the caroticotympanic artery lies in its potential supply to vascular tumors of the middle ear.
Mandibulovidian Branch of the Petrous Internal Carotid Artery
This artery is usually too small to see but may enlarge quickly in the setting of occlusive disease (see Fig. 10-13). It is unusual to see this artery in adults. When seen, it is usually in children with a vascular mass of the nasopharynx, for example, a juvenile angiofibroma. It has an origin from the horizontal portion of the petrous carotid artery. The Vidian branch is described as more horizontal and medial than the inferolateral direction of the mandibular branch. The Vidian artery has a straight course along the skull base, anastomosing with branches of the internal maxillary artery anteriorly (5).
Variant Stapedial Artery
Discussed below are the variants of the carotid artery (Figs. 10-14 and 10-15).
Cavernous Segment
From the foramen lacerum, the internal carotid artery ascends vertically and medially to the sella, where it turns anteriorly within the structures of the cavernous sinus. Anteriorly, the carotid artery makes a 180-degree turn, pierces
the proximal dural ring at the level of the anterior clinoid process, and becomes the clinoidal segment. The level of tortuosity of the carotid artery in this region is variable. Children have a straighter course than adults. In older patients, redundant superimposed loops present problems from the point of view of catheterization, visualization of the anatomy of aneurysms, and arterial injury during transphenoidal surgery.
the proximal dural ring at the level of the anterior clinoid process, and becomes the clinoidal segment. The level of tortuosity of the carotid artery in this region is variable. Children have a straighter course than adults. In older patients, redundant superimposed loops present problems from the point of view of catheterization, visualization of the anatomy of aneurysms, and arterial injury during transphenoidal surgery.
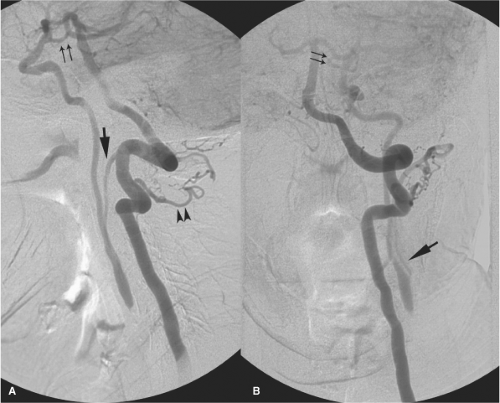 Figure 10-11. (A–B) Origin of the occipital artery from the internal carotid artery. This patient has an established occlusion of the left internal carotid artery at the level of the carotid bulb. This left vertebral artery injection fills the occipital artery (single arrow in A and B) retrogradely mainly via the C2 muscular branch (arrowheads in lateral view A). The occipital artery then flows retrogradely to fill the internal carotid artery, which then flows antegradely to the intracranial circulation. The left anterior intracranial circulation is also assisted by the posterior communicating artery (double arrows). |
Branches of the juxtasellar internal carotid artery are frequently seen with modern digital technology and may become enlarged in the presence of collateral flow or pathologic conditions (Fig. 10-16). These branches are among the most important for consideration during external carotid artery embolization. They constitute a dangerous system of anastomoses between the external carotid and internal carotid artery systems. Therefore, whether or not they are seen on an initial angiogram, embolization is always done with the cautious assumption that they are present.
The branches of the cavernous internal carotid artery supply the pituitary gland and the adjacent dura. They have important anastomoses with the distal external carotid artery and with the ophthalmic artery. They play an important role in the arterial component of dural arteriovenous malformations (AVMs). They are sometimes described as being seen as two major trunks: The meningohypophyseal trunk posteriorly and the inferolateral trunk anteriorly and laterally (Figs. 10-16–10-20). The most consistently present branches from this site are as follows.
The Marginal and Basal Tentorial Arteries
The tentorial arteries (Fig. 10-18) from this segment of the internal carotid artery are described as marginal, that is, running medially and superiorly along the margin of the tentorial incisura, or basal, that is, running laterally and inferiorly along the insertion of the tentorium along the petrous ridge.
The marginal artery of the tentorium, regardless of its many possible sites of origin, is sometimes referred to eponymously as the artery of Bernasconi and Cassinari (6). In contrast, the basal tentorial artery does not ascend in the same manner but rather diverges laterally along the course of the tentorial insertion on the petrous ridge. Along the petrous ridge and sigmoid sinus, it has anastomoses with the middle meningeal artery and dural arteries of the posterior fossa.
The Posterior Inferior Hypophyseal Artery
The posteroinferior hypophyseal artery is directed medially from the cavernous segment. It supplies the neurohypophysis and peripheral adenohypophysis of the pituitary gland. It anastomoses with the superior hypophyseal arteries (from the supraclinoidal segment), and with its contralateral
fellow. These branches cause a characteristic early neurohypophyseal blush on carotid angiography. The posteroinferior hypophyseal artery also gives a medial clival branch, which runs near the midline along the clivus to meet the ascending clival branch from the hypoglossal artery (a branch of the neuromeningeal trunk deriving from the ascending pharyngeal artery). This connection explains the occasional visualization of the pituitary blush on ascending pharyngeal artery injections.
fellow. These branches cause a characteristic early neurohypophyseal blush on carotid angiography. The posteroinferior hypophyseal artery also gives a medial clival branch, which runs near the midline along the clivus to meet the ascending clival branch from the hypoglossal artery (a branch of the neuromeningeal trunk deriving from the ascending pharyngeal artery). This connection explains the occasional visualization of the pituitary blush on ascending pharyngeal artery injections.
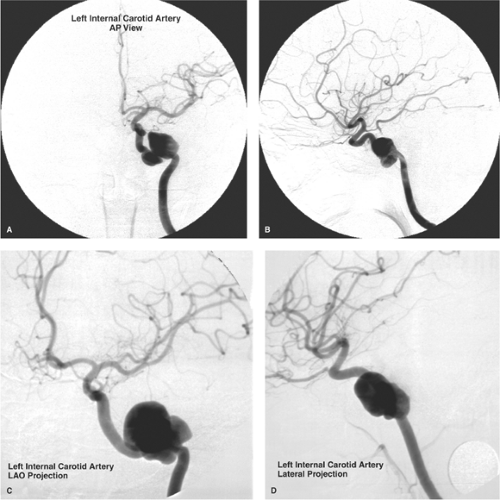 Figure 10-12. (A–D) Aneurysms of the petrous internal carotid artery. A–B: A young adult presented with symptoms of intolerable headache and left V nerve irritation. A lobulated aneurysm of the left petrous internal carotid artery was exercising considerable mass effect in the left middle cranial fossa. Previous skull trauma or petrous apicitis might be considered as possible etiologies for aneurysms in this location. A small posterior communicating artery is present (B), but the anterior communicating artery was small or absent (A). This demonstrates a need for a surgical bypass procedure before endovascular occlusion of the left internal carotid artery. The complex nature of the aneurysm, better seen on (A), presented considerable difficulties during balloon navigation, but the internal carotid artery was finally occluded at the cavernous segment. C–D: A young adult female presented with throbbing headache worsening over months. A complex aneurysm of the left petrous internal carotid artery was discovered. This patient tolerated a test occlusion of the left internal carotid artery due to the presence of a robust anterior communicating artery. However, balloon navigation of the complex lobulations of the aneurysm proved impossible, and occlusion was performed proximal to the aneurysm. Both of these cases would likely be treated today with flow-diverting devices. |
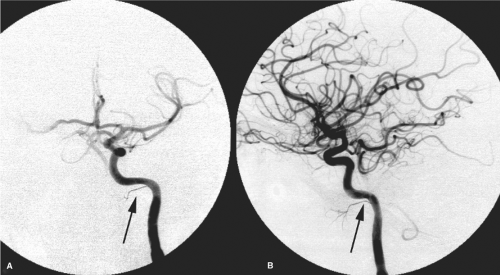 Figure 10-13. (A–B) Persistent mandibulovidian trunk. AP (A) and lateral (B) views of the left internal carotid artery in a child with a juvenile angiofibroma. An unusual branch of the petrous internal carotid artery (arrows) represents a persistent mandibular or mandibulovidian artery. |
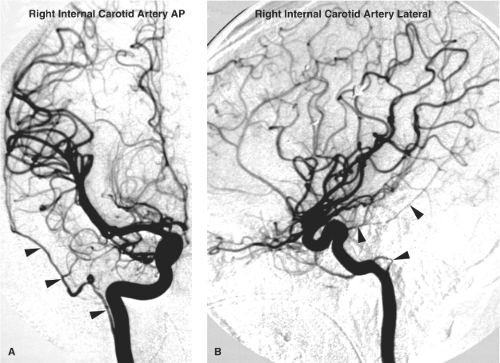 Figure 10-14. (A–B) Persistent stapedial artery variant. An AP and lateral view of the right internal carotid artery in a young adult undergoing angiography because of penetrating injury by metallic fragments after a gunshot wound. Notice the displacement of the anterior cerebral artery by hematoma on the AP view and artifact from fragments on the lateral view. An unusual vessel (arrowheads) arises from the high cervical internal carotid artery and becomes the middle meningeal artery intracranially. The lateral aspect is redolent of the curve evident when the inferior tympanic artery re-forms the petrous internal carotid artery in cases of an aberrant internal carotid artery. This particular variant has, therefore, been termed the pharyngotympanostapedial artery. |
 Figure 10-15. Variant origin of the middle meningeal artery from the petrous internal carotid artery. This patient shows a prominent and unusual variant (arrowhead) on this AP view of the left internal carotid artery. The site of origin from the petrous carotid is suggestive of this being a mandibulovidian remnant, but embryologically, the middle meningeal artery is more likely to derive variant origin through persistence of a hyoid–stapedial anomaly. |
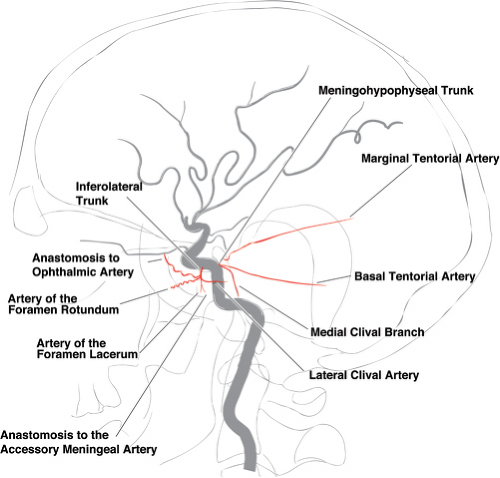 Figure 10-16. Angiographically visible branches of the cavernous internal carotid artery. |
 Figure 10-17. Meningohypophyseal trunk of the internal carotid artery. A lateral projection of the left internal carotid artery in a 60-year-old female with a large meningioma of the tentorium and petrous region. Part of the vascular supply to the tumor derives from the meningohypophyseal trunk (MHT), which supplies the tumor via the lateral clival branch. |
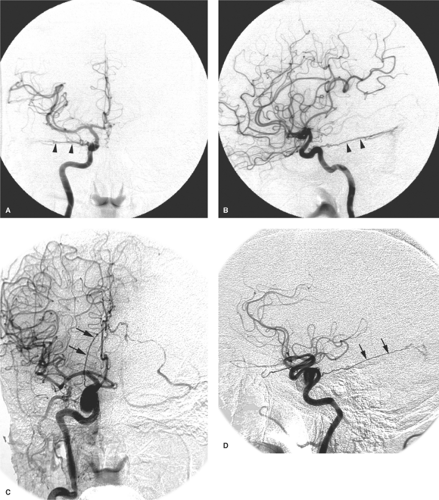 Figure 10-18. (A–D) Basal and marginal tentorial arteries. A–B: Basal tentorial artery. PA view and lateral views of the right internal carotid artery in a patient with a symptomatic dural AVM in the region of the right sigmoid and transverse sinuses. The basal tentorial artery (arrowheads) extends laterally and horizontally along the petrous ridge. This could be confirmed by looking at the course of the artery on a nonsubtracted image. C–D: Marginal tentorial artery. PA and lateral views of the right internal carotid artery in a different patient being studied for symptoms related to a cavernous internal carotid artery aneurysm. An incidental dural AVM of the tentorial margin is present. The marginal tentorial artery (arrows) follows the tentorial incisura posteriorly and superiorly. Compare with the course of the basal tentorial artery in (A) and (B). |
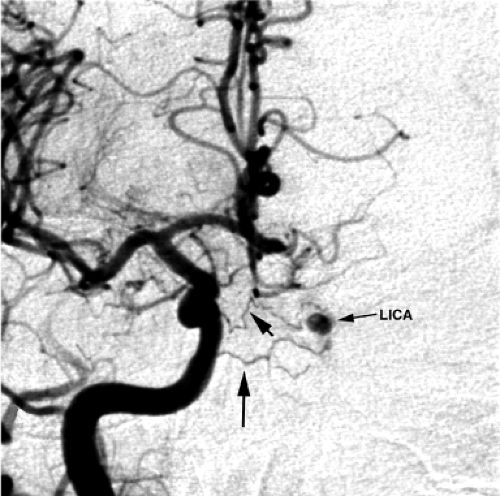 Figure 10-19. Reconstitution of the left internal carotid artery. A PA view of a right common carotid artery injection in the setting of occlusive disease of the left internal carotid artery. Early reconstitution of the cavernous left internal carotid artery (lica) is demonstrated. Small collateral vessels (arrows) cross the midline through the sella (inferior hypophyseal arteries) and along the clivus (clival branches from the internal carotid artery and ascending pharyngeal artery). |
Lateral Clival Artery
The lateral clival artery gives lateral and inferomedial branches along the course of the superior and inferior petrosal sinuses, respectively (7) (Fig. 10-17).
The Recurrent Artery of the Foramen Lacerum
The recurrent artery of the foramen lacerum is important in clinical practice by virtue of its anastomosis in the foramen lacerum with the carotid branch of the superior pharyngeal branch of the ascending pharyngeal artery.
Persistent Trigeminal Artery
The persistent trigeminal artery is discussed below with carotid basilar anastomoses.
Capsular Arteries of McConnell
The capsular arteries of McConnell in the normal state are rarely if ever seen during angiography. However, they may represent one possible site of cavernous internal carotid artery aneurysm formation. Medially directed aneurysms in this location can occupy the sella and are thought to represent a more serious variant of cavernous aneurysms. Their rupture into the sella can penetrate the diaphragm sellae and cause subarachnoid hemorrhage (Fig. 10-21). Sella-occupying aneurysms may also cause hypopituitarism as the presenting clinical problem.
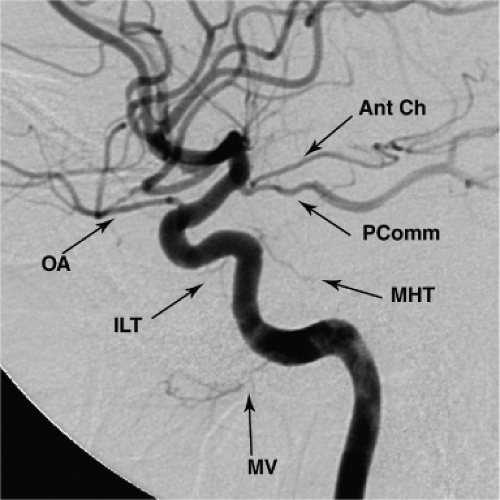 Figure 10-20. Normal anatomic branches around the carotid siphon. A lateral arteriogram in a young adult demonstrates the standard configuration most commonly seen. In the normal state, the mandibulovidian artery (MV), inferolateral trunk (ILT), and meningohypophyseal trunk (MHT) are commonly difficult to see. The dural ring can be assumed to be just proximal to the origin of the ophthalmic artery (OA), sometimes demonstrated by a cincture or subtle waist in the contour of the artery as it pierces the ring. The posterior communicating artery (PComm) and anterior choroidal artery (Ant Ch) are shown arising from their typical location. The junction of the posterior communicating artery with the posterior cerebral artery is identifiable where the vessel changes caliber, and also typically by the appearance of streaming of unopacified blood within the vessel due to laminar mixing with unopacified blood from the basilar artery. |
Inferolateral Trunk
The inferolateral trunk (8), sometimes referred to as the artery of the inferior cavernous sinus (7), is the remnant of the embryonic dorsal ophthalmic artery. It is present in more than 80% of microsurgical dissections (9) (Figs. 10-16–10-23). Its reach includes branches to the tentorium, the superior orbital fissure (potentially connecting with the ophthalmic territory), the foramen rotundum (connecting to the internal maxillary artery), the foramen lacerum (where it can anastomose with the ascending pharyngeal artery), and the foramen ovale. Very rarely, the dorsal ophthalmic artery may persist beyond embryonic life and be the dominant arterial supply to the orbit (Fig. 10-24). When a dual ophthalmic artery supply to the orbit is present (Fig. 10-25), variations in the pattern of anastomosis between the two arteries may be seen, including the possibility of a complete or partial arterial ring around the optic nerve (10).
Cavernous Carotid Aneurysms
Aneurysms of the cavernous segment of the internal carotid artery account for approximately 5% of intracranial aneurysms and are more likely to be detected in female patients (Fig. 10-26). Idiopathic aneurysms in this location have a
strong association with hypertension and advancing age, whereas posttraumatic aneurysms or pseudoaneurysms may be seen in any age group. Approximately 50% of cavernous aneurysms occur anteriorly adjacent to the carotid genu, and 16% can be giant aneurysms, that is, greater than 2.5 cm in diameter (11,12). Most cavernous aneurysms seen during angiography are incidental, asymptomatic lesions that usually warrant no further evaluation or treatment (13). Symptoms may develop due to compression of adjacent structures causing cranial nerve deficits, headache, embolic events, or aneurysmal rupture.
strong association with hypertension and advancing age, whereas posttraumatic aneurysms or pseudoaneurysms may be seen in any age group. Approximately 50% of cavernous aneurysms occur anteriorly adjacent to the carotid genu, and 16% can be giant aneurysms, that is, greater than 2.5 cm in diameter (11,12). Most cavernous aneurysms seen during angiography are incidental, asymptomatic lesions that usually warrant no further evaluation or treatment (13). Symptoms may develop due to compression of adjacent structures causing cranial nerve deficits, headache, embolic events, or aneurysmal rupture.
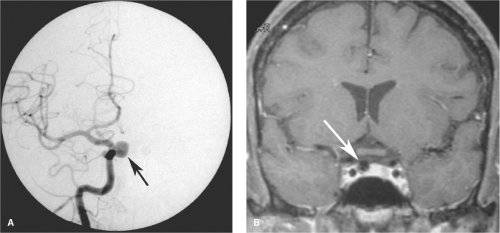 Figure 10-21. (A–B) Intrasellar aneurysm from the cavernous internal carotid artery. A PA angiographic view (A) of a right internal carotid artery injection in a middle-aged female with multiple aneurysms. A medially directed aneurysm from the cavernous internal carotid artery is present (arrow). Aneurysms in this location are thought to correspond with the hypophyseal or capsular branches. The intrasellar location was confirmed on a coronal T1-weighted, gadolinium-enhanced MRI study (B). Although this particular aneurysm was asymptomatic, endovascular treatment was recommended. Intrasellar aneurysms that rupture can leak into the subarachnoid space, causing significantly greater morbidity than rupture of cavernous aneurysms in other positions.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
