The term dementia is used in two different ways. First there are the dementias. These are diseases that cause progressive and diffuse cerebral damage, of which Alzheimer’s disease is the most common. Second, dementia can be used to refer to a clinical syndrome. Thus dementia is ‘an acquired global impairment of intellect, memory, and personality, but without impairment of consciousness’.(1) For clinicians this is the preferred usage, and the one adopted in this chapter. It demands that the cause of the dementia is explored, and makes no comment on the likely prognosis.
This chapter will focus on the management of dementia regardless of the cause; however given the burden of dementia in older age, the discussion will be invariably, but not exclusively, slanted towards the management of dementia in this age group. Aspects of management specific to individual diseases which produce dementia will be avoided. In addition, a discourse on the management of cognitive and memory problems is excluded as these are described elsewhere (see Chapters 2.5.4 and 6.2.7). Patients who suffer the dementia before 18 years of age will, by and large, not be included; their needs are often best met by services provided for people with intellectual disability.
The newly diagnosed patient with dementia
Given that it is now possible to diagnose dementia early in the course of the disease it is important to consider when and how to disclose the diagnosis. This is often seen by clinicians as a difficult task and one to be avoided until the diagnosis is absolutely certain. Stigma is associated with the diagnosis of dementia; it is perceived as a chronic debilitating illness, with a progressive deterioration in mental faculties that ultimately leads to a loss of self-identity and an unpleasant death. The clinician may believe there is not much to offer until later in disease, and so there is not much point in disclosing the diagnosis at an early stage. Furthermore, they may find it difficult to break ‘bad news’, particularly when an individual with dementia may not understand or retain information.
Nevertheless, leaving these discussions until the diagnosis is certain may be too late; the patient’s ability to take part in decisions about their future treatment, and their family’s future, may by then be jeopardized by cognitive decline. Only early in the course of the illness will they be able to make a power of attorney, settle their will, and discuss with their doctors how they wish to be treated once the disease is well advanced.
The way in which the diagnosis is given will affect how patients and their families cope and deal with the diagnosis in long-term. Although there are no specific strategies for disclosure of a dementia diagnosis, techniques developed for breaking bad news in disclosure of cancer diagnosis are probably applicable; for example, the excellent protocol devised by Baile et al.(2)
Formal psychotherapy and counselling may help patients and their families come to terms with the diagnosis.(3) Clear simple pamphlets or information sheets should be available so that patients and their families can assimilate the diagnosis and its consequences outside of the interview. Referrals can also be made to dementia support groups and local dementia societies; these can provide psychoeducation, befriending services, and networking groups for patients and their families.
After initial meeting and disclosure, it is important that a follow-up meeting is arranged; this will allow patients and families to take on board the diagnosis and formulate any questions they might have. Detailed management strategies are probably best discussed during follow-up appointments, as patients and their families might be overwhelmed at the initial appointment.
Genetic counselling and testing for dementia
Many patients and their families are concerned about the heritability of the condition and will ask if any genetic tests can be performed. But such a request needs to be considered carefully.
In only about 5-10 per cent of cases is the dementia directly due to a high penetrance genetic mutation (for example, early-onset Alzheimer’s, frontotemporal dementia, and dementia associated with Huntington’s disease). Low penetrance gene variants, such as the apolipoprotein E (APOE) genotype, while modulating, for example, the risk of development of Alzheimer’s dementia, do not adequately predict disease development. Consensus groups have therefore advised against using APOE predictive testing.(4,5and6)
There are also significant social ramifications of genetic testing for the relatives of patients with dementia; positive tests could have serious implications for employment, family planning, and insurance. Therefore access to appropriate pre-test counselling is important.
Box 4.1.13.1 shows a current modus operandi, based on United Kingdom guidelines produced by the National Institute of Clinical Excellence in dealing with this difficult subject.(4) However, the clinician is advised to keep abreast of current best practice given the likely rapid advances in this area.
The younger patient with dementia
The incidence of dementia under the age of 65 is rare. However dementia in younger people has significant additional consequences. Often the younger person with dementia has dependents and considerable financial commitments. Spouses may have to give up work to care for their partners and there are very high rates of caregiver burn-out.
Box 4.1.13.1 Guidelines for genetic testing for dementia
People likely to have a genetic cause for their dementia (for example, familial autosomal dominant Alzheimer’s disease or frontotemporal dementia, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy [CADASIL], or Huntington’s disease) and their unaffected relatives should be offered referral for genetic counselling and testing.
All patients referred for testing should have appropriate counselling in helping deal with psychological and social consequences.
If a specific genetic cause for dementia is not suspected, as is the case in late-onset dementia, genotyping should not be undertaken for clinical purposes.
Specialist service provision for the younger patient with dementia is often lacking. These patients have different life expectations than their elderly counterparts. Many will be physically fit and often do not fit easily into the service models provided for their elderly counterparts. Specialist multidisciplinary teams allied to traditional dementia services have been advocated(4) although actual implementation is still required.
Driving
Decisions about whether or not a person with dementia should be allowed to drive are often difficult. The patient’s right to autonomy needs to be balanced against their social and legal responsibilities. The clinician has a duty to consider the safety of other people on the road, as well as the patient themselves. But there is no clear consensus on the best way of making the decision, although a number of regulatory authorities have issued guidance. As a rule of thumb, patients with moderate or severe dementia should not be driving; patients with mild dementia need a careful assessment.
Advice: Begin with a history from family and relatives; this may need to be done while the patient is not present. Have there been any accidents or near accidents? Do they feel the patient is unsafe and shouldn’t be driving? A cognitive assessment (especially of executive and visuospatial function, and psychomotor speed) and physical examination of the patient is of some value although not definitive. The gold standard is a driving assessment on the road; a driving simulator test is an alternative.
Often, as in the United Kingdom, patients are legally obliged to inform their driving licensing authority about their diagnosis. The clinician should advise the patient and their relative of this, and document the discussion. Difficulties arise when a patient who is not fit to drive fails to inform the authority and continues to drive. A written warning to stop driving is often sufficient, particularly if the patient and their relatives are reminded that their car insurance policy is no longer valid. In some cases where the patient presents a real risk the clinician may need to break confidentiality and inform the authorities.
If the patient is deemed fit to continue driving, then they should be advised about risk reduction, for example keep to well-known routes and avoid busy roads, driving in bad weather conditions, or at night. They should be regularly reassessed with regard to their fitness to drive. Often this has to happen in any case because they will only be issued a short-term license (e.g. 1 year).
Behavioural and neuropsychiatric symptoms in dementia
Background
Behavioural and Psychological Symptoms in Dementia (BPSDs) have been defined by the International Psychogeriatric Association (1996) as ‘signs and symptoms of disturbed perception, thought content, mood, or behaviour that frequently occur in patients with dementia’.(7)
Identification, assessment, and management of BPSDs are central to good dementia care. These heterogeneous symptoms are highly prevalent in dementia; one study(8) found that 61 per cent of 329 patients with dementia exhibited BPSDs, with the most common symptoms being apathy (27 per cent), depression (24 per cent), and agitation/aggression (24 per cent). The presence of BPSDs is cited by carers and relatives as being the most significant determinant in generating carer stress,(9) carer burden,(10) and increasing the likelihood of subsequent institutionalization.(11)
There appears to be only a weak correlation between the level of cognitive impairment and the occurrence and severity of BPSDs. Stronger associations have been noted between the presence of BPSDs and the degree of impairment in activities of daily living.(12)
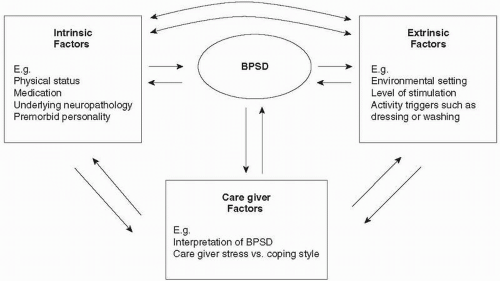
A complex interplay of factors can give rise to these symptoms and include intrinsic host attributes and extrinsic environmental influences (Fig. 4.1.13.1). Therefore the same symptom in different individuals may be due to different causes. For example, aggression may be the response to a delusion in one individual, and the reaction to a change in caregiver in another. Often several different problem behaviours are seen in the same patient, such as wandering and sleep disturbance. There may be causal links between different BPSDs, for example the presence of distressing auditory hallucinations and persecutory delusions is strongly associated with consequent aggression.(13) Particular constellations of BPSDs are often associated with specific dementia syndromes (Table 4.1.13.1). BPSDs will change over time; for example aggression and psychosis tend to occur in the early to middle stages of Alzheimer’s dementia whereas incontinence is invariably a feature of late disease.
Of all the symptoms that patients with dementia suffer, it is the problems caused by BPSDs that are most likely to trigger a pharmacological intervention or institutionalization. But whether or not a BPSD is reported as being a problem depends heavily on the informant and the situation. For example, night-time wandering may be tolerated by the spouse with the patient in their own home, but not by nursing staff in an acute medical ward.
Assessment
Assessment of a BPSD begins with a carefully taken informant history to assess the nature, history, and severity of the BPSD, and to garner the background medical, psychiatric, and social history. For example, there may be a history of phobic disorder, which is now manifest as agitation, or a lifelong tendency to aggression. Alcohol or other drug abuse must be addressed. The effect of recently prescribed, and recently stopped, medications needs to be considered. The impact of the BPSD on the patient and the carer should be determined. Consider environmental influences; ask when the BPSD first occurred and whether it now occurs at any specific time, and whether it is related to any prior activity or antecedents. This will aid in formulation of specific behavioural management strategies (see below).
Fig. 4.1.13.1 Interaction between intrinsic host factors, extrinsic factors, and caregiver factors in the aetiology of BPSDs.
The mental state examination will look for evidence of anxiety, depression, or psychosis and persecutory delusions, and ascertain the patient’s insight and understanding of their behavioural/ neuropsychiatric symptoms. With specific problem behaviours direct observation of the behaviour can be very useful. A thorough physical examination will be needed to exclude physical illnesses; if suspected then appropriate medical investigations should be considered such as a midstream urine sample or chest X-ray. In agitated behaviours, sources of pain and fear should be considered, as well as the possibility of sleep loss or constipation, cold, or hunger. The presence of any sensory deprivation (e.g. hearing loss) should be looked for. Conversely the patient may be over-stimulated, as commonly occurs on general medical or surgical wards because of the noise and hustle and bustle.
Table 4.1.13.1 Common BPSDs in major dementia syndromes
A range of objective instruments for the measurement of BPSDs now exist.(14) Some measure multiple domains, for example the Behavioural Pathology in Alzheimer’s Disease rating scale.(15) Other instruments are specific for one symptom, such as the Cohen-Mansfield Agitation Inventory(16) or Cornell scale for depression in dementia.(17) There are several caveats to the use of such scales, including the large intra-individual variations in scale scores which reflects the dynamic nature of BPSDs and variable reporting patterns of different observers. Some scales take a long time to complete or require training to administer. Nevertheless in clinical practice, the judicious use of such scales can allow for more reliable assessment of the response to a specific behavioural or pharmacological intervention.
Management of agitation and challenging behaviour
Agitation includes behaviour that is aggressive or abusive and occurs at an inappropriate frequency or is socially inappropriate.(18) Challenging behaviour has been used as a ‘catch all’ for a number of different behaviours including aggression, combativeness and disruptive vocalizations and may or may not be associated with agitation.
(a) Behavioural interventions
Evidence: Research into the effectiveness of behavioural techniques for agitation and challenging behaviour is based largely on studies using A-B-A-B or single-case design, and case series. Recent systematic reviews suggest that individually tailored behavioural interventions are effective.(19,20,21and22)
Advice: An intervention programme would start with a situational, or ABC, analysis:
Antecedents—what was happening before the behaviour started?
Behaviour—a clear description of the behaviour.
Consequences—what happened as a result of the behaviour, particularly looking for possible reinforcers of the behaviour?
The frequency and severity of the behaviour then need to be charted as a baseline before introducing the specific intervention. Many programmes rely on the differential reinforcement of other behaviour (DRO); this involves positive reinforcement of other, appropriate behaviours, with the hope that these will then replace the challenging behaviour. A useful technique to be used alongside DRO is ‘time out on the spot’ (TOOTS), in which the unwanted behaviour is met with immediate withdrawal of social contact; appropriate behaviours receive warm social contact.
Unfortunately the limiting factor in use of behavioural interventions in dementia is the lack of trained individuals; often behavioural programmes can only be implemented in specialist units. In addition, the whole nursing/multidisciplinary team must be aware of the principles of reinforcement and extinction of behaviour, because behavioural programmes are unlikely to be effective unless consistently applied across the team. Evidence for the effectiveness of educating carers/family members in behaviour management techniques is currently inconclusive.(22) An alternative view which is gaining prominence is that while some challenging behaviours may not be amenable to interventions, it is possible to change the caregiver perception of the problem; this can lead to a reduction in caregiver distress and often by improving an aberrant interaction between caregiver and patient, there is a reduction in the challenging behaviour itself.
Table 4.1.13.2 Psychosocial interventions in dementia
Intervention
Description
Evidence for effectiveness
Psychoeducation to staff
Educating staff about dementia, neuropsychiatric symptoms, and reduced use of restraint
Possibly effective—might have sustained benefits
Reminiscence therapy
Uses materials related to patient and their era for example, old photographs and news articles, to stimulate memories and allow sharing of experiences
Possibly effective
Cognitive stimulation
Similar to reality orientation therapy, based on information processing rather than orientation knowledge
Possibly effective—might have sustained benefits
Music therapy
Can consistent of playing music as part of activity sessions or at specific times of the day. Music often of patient’s era
Possibly effective—but no evidence of prolonged benefit
Snoezelen/multi-sensory therapy
Combined relaxation and use of sensory stimuli e.g. sounds, lights, touch
Possibly effective—but benefit wears off quickly. Also time/staff intensive
Aromatherapy
Mostly using lemon balm oil and lavender oil either inhaled or applied by massage
Possibly effective for agitation and restlessness
Bright light therapy
Sustained exposure to high levels of light (up to 10000 lux)
Possibly effective (may be more benefit in sleep disturbance than behavioral disturbance). Time/ staff intensive
Pet therapy
Contact with animals
Inconclusive
Exercise
Walking or light exercise sessions
Inconclusive
Simulated presence
Audiotape recorded by caregiver/family member played to patient where positive autobiographical memories are reiterated
Not effective
Reality orientation
Regular provision of orientating information e.g. time, date, etc.
Not effective
Validation therapy
Rogerian-based therapy; allowing resolution of unfinished conflicts, the acceptance of the reality and the expression of feelings
Not effective
Only gold members can continue reading. Log In or Register to continue