CHAPTER 6 THE NEGLECT SYNDROME
There are few more dramatic sights in clinical neurology than a patient ignoring one half of his or her environment, including one half of a meal, or insisting that a paretic left arm is entirely normal, while that held by the examiner must belong to someone else. These examples of severe neglect syndromes, manifest by spatial neglect, and personal neglect with anosognosia (denial of deficit), respectively, are uncommon and a suitable subject for medical literature.1 However, lesser degrees of the neglect syndrome are common, especially in right hemisphere stroke, and have an adverse effect on prospects for rehabilitation and function. Therefore, any practicing neurologist likely to encounter patients with acute or subacute hemispherical lesions—the typical cause of the neglect syndrome—must be aware of its possible manifestations and must be able to confirm their presence at the patient’s bedside.
The neglect syndrome is a constellation of related lateralized deficits, including neglect of sensory stimuli; extinction of awareness of one sensory stimulus by another when both are delivered simultaneously; neglect of one half of an object or of space (recognizing that different reference points for “left” exist in this context); neglect of part of a person’s own body; failure to move a (nonparetic) body part as rapidly or persistently as its contralateral equivalent; and failure to recognize that the function of one part of the body is, indeed impaired.2 Although many of these features tend to occur together in individual patients, they are potentially dissociable, and each patient must have his or her own distinctive pattern of impaired and retained abilities elucidated and documented, to facilitate further monitoring, care, and rehabilitation.
TERMINOLOGY AND PHENOMENOLOGY
The various components of the neglect syndrome each have their own descriptive terms; because patients may exhibit a wide range of combinations of these individual deficits, it would be as inappropriate to lump these together as “neglect” as it would be to refer to all disorders of central language processes as “aphasia” without further qualification. The reader interested in a more detailed exposition of each of the elements of the neglect syndrome is referred to Heilman and colleagues (2003). The following classification is somewhat arbitrary—for example, neglect dyslexia might conceivably also be regarded as a motor disorder, and spatial neglect might legitimately be considered “sensory”—but some form of organization, even imperfect, is probably useful in considering the wide range of deficits subsumed under “neglect”.
Sensory Aspects of the Neglect Syndrome
Sensory Neglect
Sensory neglect is said to exist when the patient is not consciously aware of or able to respond to a sensory stimulus contralateral to the lesion, in the absence of a deficit in the relevant sensory pathways or its cortical projections sufficient to prevent apprehension of the stimulus. This defect can be unimodal, but it may affect vision, touch, hearing, and even olfaction together. It can, of course, be difficult to determine whether a patient has neglect or a primary sensory disturbance. However, as pointed out by Heilman and colleagues (2003),2 the bilateral nature of the central auditory pathways makes the diagnosis of auditory neglect easy: A patient with unilateral deafness will hear a sound applied to their deaf side in their good ear if the sound is loud enough, and unilateral cortical lesions typically do not cause deafness. Complete hemianesthesia is uncommon with hemispherical lesions, apart from those involving the thalamus. A patient with a thalamus-sparing cortical lesion who has hemianesthesia probably actually has sensory neglect. The olfactory pathways are uncrossed. Hemianopia, particularly hemianopia plus neglect, is the most difficult to distinguish from hemineglect alone.2,3 Patients with hemianopia without neglect are often aware of and compensate for their deficit, deliberately scanning into their area of field loss, but even the use of examination techniques such as supramaximal stimuli (e.g., bright torch in a dark room) may leave room for doubt.
Extinction
Extinction (or sensory extinction to double simultaneous stimulation) is said to be present when the patient does respond to sensory stimulation on the contralesional side but then fails to do so when another stimulus is applied simultaneously. The extinguishing stimulus is typically similar to that being extinguished and is usually applied to the corresponding contralateral area, but transmodal extinction (e.g., of a left-sided tactile stimulus by a right-sided visual stimulus) can occur, as can extinction of one stimulus by a second ipsilateral stimulus. When this occurs, the rightward stimulus typically extinguishes that further to the left: this allocentric effect can be seen in the ipsilesional as well as the contralesional receptive field. Extinction, too, may be unimodal or multimodal.
Spatial Aspects of the Neglect Syndrome
Spatial Neglect
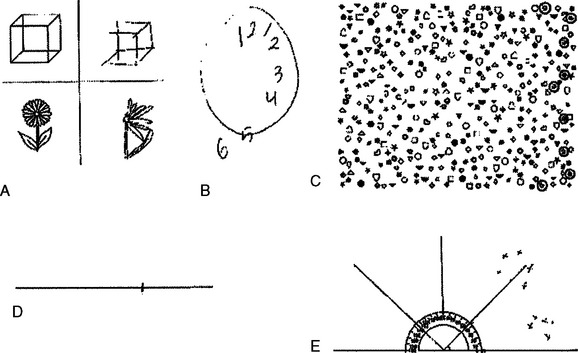
Spatial neglect refers to decreased awareness of contralesional hemispace. However, what constitutes “hemispace” depends on the frame of reference. Patients may neglect the left side of retinocentric space (i.e., the left side of wherever they are looking), the left side of cephalocentric or somatocentric space (referable to the direction of the head or body), or the left side of environmental space (in relation to an environmental fixed point). For example, patients with neglect of somatocentric hemispace who turn their heads and eyes to the right bring their left visual field into the right side of space, as defined in relation to a somatocentric reference point. This improves their detection of left-sided visual stimuli (defined in relation to a retinocentric reference point) and may help the clinical distinction from hemianopia. A patient with left environmental-centered neglect who lies on his or her left side would neglect stimuli toward the feet. Spatial neglect also occurs for only peripersonal (near) space (i.e., what can be reached) and, less commonly, for far space, or for both together. A related concept is that of spatial neglect for object-centered (allocentric) space. This refers to a tendency to ignore the left sides of objects, regardless of where they are in retinocentric, somatocentric, or environmental space (Fig. 6-1).4 In addition to neglecting half their environment, such patients may also display neglect dyslexia, in which there is a tendency to ignore the left parts of words (e.g., misreading “consequence” as “sequence”) or of lines. This is an unlikely occurrence in hemianopia without neglect.
Representational Neglect
Representational neglect refers to the neglect of the left side of mental images. This disorder first became widely recognized as a result of a thought experiment in which patients imagined themselves standing in the Piazza del Duomo in Milan.5 If they imagined themselves standing on the steps of the cathedral, they could recall the buildings on their right in greater detail than those on the left. If they then imagined themselves standing at the opposite end of the square looking back at the cathedral, they could now recall those buildings previously on their left (but now on their right) in greater detail than those previously on their right (but now on their left).
Body Image Aspects of the Neglect Syndrome
Anosognosia and Anosodiaphoria
The reader might intuitively suspect that anosognosia (denial of deficit, such as hemiparesis), or the less severe but similar anosodiaphoria (lack of appropriate concern regarding an admitted deficit) is related to personal neglect; however, anosognosia can certainly exist in the absence of personal neglect.6 Of course, neither anosognosia alone nor anisodiaphoria alone is necessarily part of a neglect syndrome: both can occur in other circumstances (e.g., denial of cortical blindness in Anton’s syndrome, la belle indifference in conversion disorders).
Motor Aspects of the Neglect Syndrome
Motor neglect, in a broad sense, refers to a situation in which patients fail to perform an appropriate movement, despite awareness of the imperative stimulus and preservation of the requisite power. It is usually implicit that the disorder does not just affect skilled movements, inasmuch as this could then be classed as an apraxia. Heilman and colleagues classified these deficits as action-intentional disorders and recognize four types: akinesia, motor extinction, hypokinesia, and motor impersistence.2 Akinesia refers to failure of initiation of movement. If this failure of initiation is in response to an external stimulus, it may be also be termed motor neglect (in a narrower sense). Akinesia may vary, depending on in which part of peripersonal space the movement occurs and on in which direction the movement is made. For example, akinesia of the left hand may be less severe if movements are attempted in right hemispace (e.g., with the hands crossed), and the ipsilesional (right) hand may move less freely to the left side. Ingenious experiments, designed to separate motor from sensory/hemispatial neglect, have been reported. Perhaps one of the simplest is the crossed response task, in which a stimulus in the right hemifield requires movement of the left arm, and that in the left hemifield requires movement of the right arm.2 Motor extinction is analogous to sensory extinction: a limb that can move normally in isolation moves less well when the opposite limb is moved at the same time. Hypokinesia refers to a normally executed movement with an abnormally long delay from stimulus to movement onset (reaction time). This delay may be long enough to be obvious clinically. Inability to sustain a motor act constitutes motor impersistence. This may be directional (e.g., inability to keep looking in the contralesional but not ipsilesional direction) or may affect the contralesional arm or whichever arm is in contralesional hemispace.
How Separable Are the Various Components of the Neglect Syndrome?
The neglect syndrome has long been recognized to consist of various combinations of the constituent deficits outlined previously. Formal double dissociations have been recorded between a number of the components (e.g., different measures of hemispatial neglect; hemispatial neglect and extinction).7,8 The best evidence for the heterogeneity of the syndrome probably comes from the large study of Buxbaum and coworkers, who found most possible combinations of personal neglect, peripersonal spatial neglect, sensory neglect/extinction (“perceptual neglect”), and motor neglect in their sample of 166 patients with right hemisphere stroke.9 Pure personal neglect was rare, but pure peripersonal spatial neglect, pure sensory neglect, and pure motor neglect were each not uncommon. Of course, their “purity” depends on which tests are chosen for each, together with their psychometric characteristics, but the double dissociations observed still stand.
EXAMINATION FOR THE NEGLECT SYNDROME
It is apparent from the preceding section that no one test is adequate for ruling out the neglect syndrome. At the same time, a relatively brief bedside assessment readily detects most clinically significant neglect syndromes. Several batteries of appropriate tests have been developed.10,11 The following outline is condensed predominantly from Heilman and colleagues (2003), to which the reader is referred for further details.
Sensory Aspects
The patient should be stimulated on the left side, right side, and on both sides together, in random order, with visual, tactile, and auditory stimuli and asked to state or indicate on which side or sides the stimulus occurred. Verbal misreporting of left as right, despite absence of left-right confusion on other measures (e.g., the patient can point to and/or move the appropriate side as requested), suggests allesthesia. As pointed out previously, auditory neglect or extinction is clearly separable from unilateral deafness, or unilateral involvement of auditory cortex, and nonthalamic lesions typically do not cause complete hemianesthesia, but it can be more difficult to separate visual hemineglect from hemianopia. Confrontational field testing should then be performed with the head turned to the right and to the left: a true hemianopic defect should remain retinocentric, but visual neglect may improve with the head’s turning to the right. Stronger stimuli should also be employed (e.g., a torch, the spot of a laser pointer on the wall in a darkened room, or, at least, targets larger than a hat pin). Sometimes, however, it is difficult to be certain of with what the clinician is dealing.3 Visual extinction of the more central stimulus by that further to the right may be demonstrable in the intact field.3
Spatial Aspects
Gross degrees of spatial neglect are evident on observation: the patient disregards the left side of the environment. Asking the patient to report 10 objects around their room (provided that the bed is not against the left wall) and marking these with regard to a patient-centered reference frame can be a useful measure of less severe spatial neglect (Fig. 6-2E).3 Persistent head and/or eye deviation to the right may also offer a clue to lesser degrees of neglect, which may be elicited by a number of pencil and paper tests. Object drawing/copying tests (see Fig. 6-2A and B) are traditionally used but are not particularly sensitive by themselves,12 are difficult to quantify, and may be confounded by other visuoconstructional problems. A number of cancellation tests have been devised. Those with dense, random arrays with many different types of distractor items, such as the Bells Test,13 or Mesulam’s shape cancellation test (Fig. 6-3; see also Fig. 6-2C),14 seem to be the most sensitive.2,3 A starting point toward the right of the array is probably the most sensitive measure,12 and the location of the first item canceled should be noted. The left-minus-right omission score is also noted: a cutoff point of greater than 2 has been used on the Bells Test, for example.12
< div class='tao-gold-member'>






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


