CHAPTER 37 The Posterior Petrosal Approach for the Treatment of Petroclival Meningiomas
OPERATIVE TECHNIQUE
Craniotomy Flap
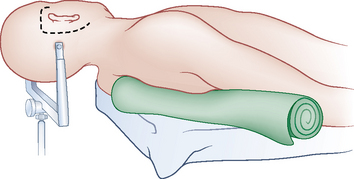
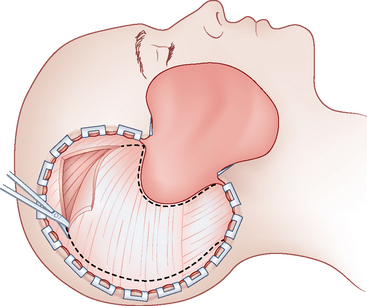
The skin incision is made extending from the zygoma anterior to the tragus, and extending in a curvilinear fashion behind the ear to below the mastoid process (Fig. 37-1). The skin flap is rotated anteriorly and inferiorly, and the temporal fascia is incised and reflected inferiorly in continuity with the sternocleidomastoid muscle. The temporalis muscle is cut along the superior edge of the incision and retracted inferiorly and anteriorly (Fig. 37-2). This flap will be used at the time of closure to cover the drilled surface of the temporal bone. Once these maneuvers are complete, the bony surfaces of the temporal fossa, mastoid, and lateral posterior fossa are exposed.
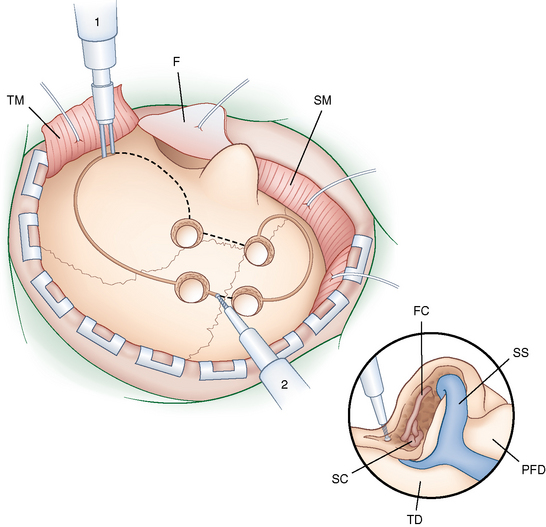
Four burr holes are placed straddling the transverse sinus, two in the posterior fossa and two supranteriorly. One hole is made just medial and inferior to the asterion opens into the posterior fossa below the transverse–sigmoid sinus junction. Another hole located at the squamal and mastoid junction of the temporal bond along the projection of the superior temporal line opens into the supratentorial compartment. A single bone flap covering the middle and posterior fossae is made using the foot attachment of a high-speed drill using the burr holes on either side of the sinus for access. The burr holes flanking the sinus are then connected using a rongeur or the drill. Caution should be taken during this step to avoid injury to the venous sinus wall during this step. The transverse–sigmoid sinus junction is exposed with the craniotomy. Care should also be taken when removing the bone flap because in many patients the bone is very adherent to the dura at the junction of the transverse and sigmoid sinus (Fig. 37-3).
Temporal Bone Drilling
Before drilling the mastoid air cells, the mastoid cortex is scored and cut. This mastoid cortex will be used to reconstruct the calvarium at closure. At this point, the surgeon performs a complete mastoidectomy. This may be started using a round cutting burr; however, we recommend using a diamond bit when drilling near vital anatomic structures. The sigmoid sinus is skeletonized to the jugular bulb. The sinodural angle, Citelli’s angle, which denotes the position of the superior petrosal sinus, is exposed. The superficial mastoid air cells behind the posterior wall of the external ear canal as well as the deep retrofacial air cells are resected to identify the facial canal and the lateral and posterior semicircular canals. Drilling is carried forward along the pyramid to thin the petrous bone toward the apex. Care is taken at this step to leave the facial canal as well as the middle and inner ear structures intact (see Fig. 37-3, inset).






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


