The Venous System
Key Points
Venous anatomy can vary a great deal meaning that the clinical impact of venous pathology or excessive venous flow can be very variable from one patient to another.
Many of the venous connections between the petrosal sinuses and the pial veins have an arcane nomenclature, but these connections are very important in the genesis of venous complications from remote arteriovenous fistulae.
The venous system of the intracranial and extracranial structures of the neck and head is most easily described in separate spaces or compartments. However, it is important to understand the remarkable potential of these layers to communicate. The variable pattern of free communication through certain channels, in combination with selective flow restriction through others, forms the basis for the pathophysiology of some vascular diseases of the brain and its coverings. A small shunt or fistula in a certain setting can have a catastrophic clinical effect on one patient; another patient with a large shunt in the same location may be asymptomatic and may even be best left untreated.
Extracranial Veins
The scalp and face are highly vascular structures with a rich network of large veins throughout. The superficial temporal vein corresponds with the artery of the same name and runs down anterior to the ear to the posterior aspect of the parotid gland (Figs. 16-1 and 16-2). Here, it usually joins with the internal maxillary vein to form the retromandibular vein. The retromandibular vein joins the internal jugular vein. The anterior facial vein may also join the retromandibular vein or may empty directly into the internal jugular vein. The angular vein is formed at the junction of the frontal and supraorbital veins and forms an important anastomosis posteriorly with the superior ophthalmic vein. Although it usually drains inferiorly into the facial vein, it can drain into the cavernous sinus if flow is reversed and can become a conduit for propagation of infection or thrombosis. The occipital vein drains inferiorly into the deep cervical or vertebral veins. It may connect with the posterior auricular vein, and then to the external jugular vein.
The intracranial and extracranial venous systems communicate via emissary veins through skull foramina. Important emissary veins connect the superior sagittal sinus and transverse sinus with the suboccipital veins. The pterygoid plexus lies outside the skull base but has a number of important connections with the cavernous sinus via the foramina of the middle cranial fossa, notably the foramen of Vesalius, the foramen ovale, and other foramina innominata (Figs. 16-3 and 16-4). The pterygoid plexus usually drains to the facial vein. It may also connect superiorly into the orbit via the inferior orbital fissure through which it drains part of the inferior ophthalmic vein.
The internal jugular vein runs inferiorly in a position lateral to the internal carotid artery. The internal jugular vein receives input from the inferior petrosal sinus, the facial vein, the lingual vein, the pharyngeal veins, and the thyroidal veins. In the thoracic inlet, it joins with the subclavian vein to form the brachiocephalic vein.
The external jugular vein receives venous outflow from the scalp, occipital region of the neck, and part of the face. It forms in the parotid gland and runs inferiorly superficial to the sternocleidomastoid muscle.
The vertebral vein forms at the level of atlas and runs as a plexus in the foramina transversaria surrounding the vertebral artery. A single outlet vein runs inferiorly and then joins the brachiocephalic vein.
Meningeal Veins
Meningeal veins accompany their respective meningeal arteries. The anterior meningeal vein joins the superficial Sylvian vein to form the sphenoparietal sinus. The sphenoparietal sinus then passes below the lesser wing of the sphenoid bone to join the cavernous sinus. Alternatively, it may course posteriorly in the middle cranial fossa to join the lateral sinus.
Dural Sinuses
The dural sinuses are venous channels enclosed between two layers of dura. They do not have valves.
The superior sagittal sinus extends from the foramen cecum to the torcular herophili (Fig. 16-2). Occasionally, the superior sagittal sinus may bifurcate above the internal occipital protuberance. The superior sagittal sinus drains the superficial cerebral veins from the lateral and medial surfaces of the cerebral hemispheres. The largest such
named vein is the vein of Trolard. Venous lacunae along the course of the superior sagittal sinus contain arachnoid granulations, which become more prominent with age. They may form filling defects within the sinus itself. Veins entering the superior sagittal sinus often appear constrained at the point of entry, giving a false appearance of venous stenosis.
named vein is the vein of Trolard. Venous lacunae along the course of the superior sagittal sinus contain arachnoid granulations, which become more prominent with age. They may form filling defects within the sinus itself. Veins entering the superior sagittal sinus often appear constrained at the point of entry, giving a false appearance of venous stenosis.
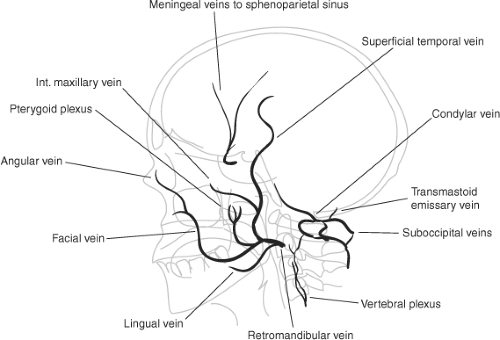 Figure 16-1. Superficial extracranial and middle meningeal veins. |
The torcular herophili, named for its similarity to the handle of a manually operated winepress (1), is the confluence of the superior sagittal sinus, the straight sinus, and the occipital sinus. It drains into the two transverse sinuses. The drainage is usually bilateral. If unilateral or asymmetric, the right transverse sinus is usually larger (2).
The inferior sagittal sinus lies along the inferior edge of the falx cerebri. It drains the anterior part of the corpus callosum, the medial portions of the cerebral hemispheres, and the falx. It joins with the internal cerebral vein to form the vein of Galen.
The straight sinus extends posteriorly from the junction between the falx cerebri and the tentorium, where it collects the vein of Galen and related tributaries. It drains to the torcular posteriorly.
The occipital sinus is inconstantly seen (Figs. 16-2B and 16-5). It usually drains upward to the torcular. It may flow inferiorly and bevel laterally to join the sigmoid sinus or connect with a sinus around the foramen magnum, termed the marginal sinus. The occipital and marginal sinuses are most commonly seen in young children. They diminish in size with age.
The transverse (lateral) sinuses curve laterally in the perimeter of the tentorium until they turn inferiorly to form the sigmoid sinuses. The transverse sinus receives a number of important supratentorial veins from the temporal and occipital lobes, notably the vein of Labbé. Infratentorial veins also drain to the transverse sinus, and it also receives the drainage of the superior petrosal sinus.
The sigmoid sinus represents the anterior, medial, and inferior continuation of the transverse sinus. It becomes the internal jugular vein in the jugular fossa and may receive direct venous channels from the pons and medulla. It communicates with the scalp veins via the mastoid and condylar veins.
The superior petrosal sinus runs from the posterior aspect of the cavernous sinus along the petrosal ridge to the junction of the sigmoid and transverse sinuses within the basal attachment of the tentorium. It receives venous channels from the supratentorial and infratentorial compartments and from the tympanic structures. It may lie either adjacent to or surround the roots of the trigeminal nerve.
The inferior petrosal sinus runs inferiorly and laterally from the posterior part of the cavernous sinus to join the jugular vein in the pars nervosa, which it shares with the glossopharyngeal nerve. The inferior petrosal sinus may receive channels from the medulla, cerebellum, and internal auditory veins.
The sphenoparietal sinus drains the superficial Sylvian vein into the cavernous sinus along the lesser wing of sphenoid behind the orbit. It receives variable contributions from meningeal, orbital, medial anterior temporal (uncal), and inferior frontal veins. Less commonly, this venous system may not reach the cavernous sinus. Alternatively, it can turn posteriorly in a sinus, most commonly referred to as the sphenopetrosal sinus (3), running along the floor of the middle cranial fossa to drain along the tentorium and into the superior petrosal sinus. An alternative variant drains into the pterygoid plexus and bypasses the cavernous sinus.
The cavernous sinus represents the most important site of confluence of intracranial and extracranial venous structures. Variations in the configuration of the outlets from the cavernous sinus are of little significance in the normal state. However, in the setting of pathologically increased blood flow through the sinus, the varied nature of the resulting clinical conditions is determined by the restrictions on venous outflow from the cavernous sinus.
Orbital venous drainage is via the superior and inferior ophthalmic veins, normally in an anterior to posterior direction.
There are important variable anastomoses anteriorly with angular branches of the facial vein and frontal veins. The superior ophthalmic vein communicates posteriorly with the cavernous sinus and occasionally with the sphenoparietal sinus. The inferior ophthalmic vein also connects anteriorly with the facial vein and drains posteriorly to the cavernous sinus separate from or after joining the superior ophthalmic vein. It also connects inferiorly via the inferior orbital fissure with the pterygoid plexus.
There are important variable anastomoses anteriorly with angular branches of the facial vein and frontal veins. The superior ophthalmic vein communicates posteriorly with the cavernous sinus and occasionally with the sphenoparietal sinus. The inferior ophthalmic vein also connects anteriorly with the facial vein and drains posteriorly to the cavernous sinus separate from or after joining the superior ophthalmic vein. It also connects inferiorly via the inferior orbital fissure with the pterygoid plexus.
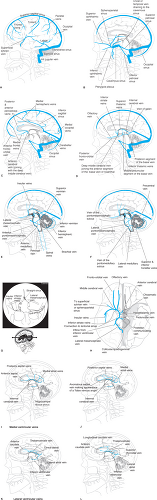 Figure 16-2. (A–D) Intracranial dural sinuses and veins. A: Superficial cortical veins of the left hemisphere are illustrated. A balanced arrangement of the superficial Sylvian vein, vein of Trolard, and vein of Labbé is depicted. B: The left hemisphere has been removed from the illustration. The left superficial Sylvian vein is still in place (from A) to illustrate its relationship to the cavernous sinus. An understanding of the variability of the connections to and from the cavernous sinus is important to explain the clinical and angiographic consequences of arteriovenous shunting in this structure. The most common connection of clinical consequence is to the superior ophthalmic vein. A sinister possibility is the presence of connections from the cavernous sinus to the basal vein. Venous hypertension transmitted through this route accounts for the most serious complications of such disorders. C: Superficial veins close to the midline are illustrated. The anterior pericallosal vein becomes the anterior cerebral vein. This vein may communicate across the midline via the anterior communicating vein. The anterior cerebral vein usually joins the anterior segment of the basal vein. D: The major components of the deep venous system are illustrated. E–H: The insular veins, which are defining tributaries of the middle cerebral vein, usually superimpose on the inferior striate veins and are illustrated in (E) and (H). The internal cerebral vein runs in the velum interpositum; it should therefore be superimposed on the course of the medial posterior choroidal artery from the arterial phase of the posterior circulation. E and F: The insular veins are demonstrated without the underlying inferior striate veins. The major anastomotic vessels of the posterior fossa are illustrated. G: A schematic illustration of the shape of the basal vein and middle cerebral vein as seen on a Townes projection. The segments of the basal vein are numbered I, II, and III. The lateral mesencephalic vein slopes medially along the surface of the midbrain. Therefore, it usually has a characteristically medial course relative to the basal vein, demonstrated on the anatomic left side here. It drains to the superior petrosal sinus via the petrosal vein. H: A base view of the brain demonstrates the complete territory of the basal vein. In reality, it is common for the basal vein to be a fragmented structure with preferential drainage through alternative pathways other than the vein of Galen. I–L: I, J: The outline of the lateral ventricle is depicted by the dotted line. The medial ventricular veins are demonstrated in lateral appearance. It is rare to identify the hippocampal veins unless there is a high flow state such as might be related to the presence of an AVM. The inferior ventricular vein runs in the roof of the temporal horn and connects with the veins on the lateral wall of the atrium. K and L: The lateral ventricular veins of the deep system are illustrated in lateral projection. |
The cavernous sinuses are multicompartmental extradural spaces that lie on either side of the sella on the surfaces of the greater wing of the sphenoid bone. They are interconnected by the anterior and posterior coronary (intercavernous) sinuses under the diaphragm sellae and by variable sinuses on the clivus (Fig. 16-3). Anteriorly, they accept venous drainage from the ophthalmic veins and the sphenoparietal sinus. Posteriorly, they can accept parenchymal draining channels from the temporal lobe, particularly the uncal vein or middle cerebral vein. They also receive flow from the hypophyseal veins.
Outflow from the cavernous sinuses is mainly posteriorly to the petrosal sinuses. There are also draining connections to the pterygoid plexi through the foramina of the middle cranial fossa. The superior petrosal sinus and inferior ophthalmic vein may be either afferent to or efferent from the cavernous sinus.
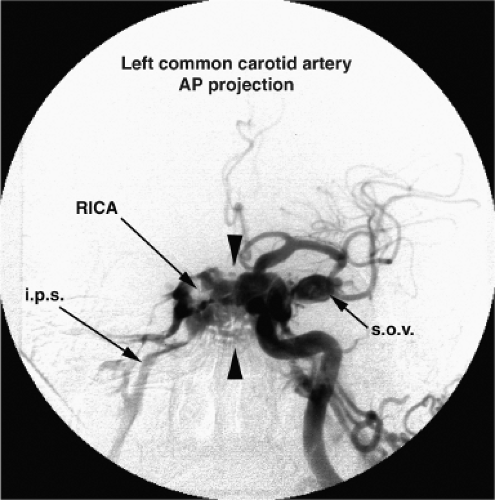 Figure 16-3. Intercavernous venous connections in a dural AVM of the left cavernous sinus. A left common carotid artery injection opacifies a multitude of venous structures in the region of the left cavernous sinus through involved branches of the external carotid artery. Prominent intercavernous connections through the sella and along the clivus connect across the midline (arrowheads) to opacify the right cavernous sinus. Within the latter, lucency is preserved by the course of the unopacified right internal carotid artery (RICA). Prompt drainage to the right inferior petrosal sinus (i.p.s.) is seen. On the left side, the superior ophthalmic vein (s.o.v.) is massively distended. It projects foreshortened along the plane of viewing. |
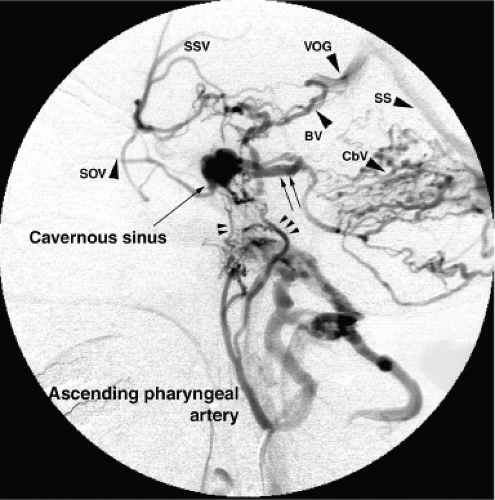 Figure 16-4. Venous hypertension due to restricted outflow from the cavernous sinus. Unlike the patient in Figure 16-3, this patient with the same diagnosis, dural AVM of the cavernous sinus, does not have ready outflow from the cavernous sinus to the contralateral side or to the superior ophthalmic vein. At least, this is the case for the involved compartment of the cavernous sinus. This injection is made into the ascending pharyngeal artery in the lateral projection. There is early opacification of the cavernous sinus via the carotid branch of the pharyngeal trunk (double arrowhead) and clival branches (triple arrowhead) from the neuromeningeal trunk. The superior ophthalmic vein (SOV) is small. The cavernous sinus decompresses itself via the basal vein (BV) with connections to the Sylvian veins (SSV), the vein of Galen (VOG), and the straight sinus (SS). There is prominent opacification of cerebellar veins (CbV) in the posterior fossa. This is because of drainage from the cavernous sinus via the superior petrosal sinus (double arrow). The patient’s symptoms were related to venous hypertension of the posterior fossa. |
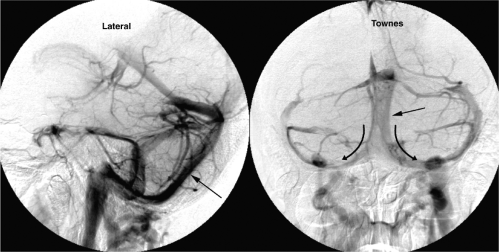 Figure 16-5. Prominent occipital sinus. An incidental observation of a large occipital sinus in an adult patient. The occipital sinus (arrows) descends along the falx cerebelli and divides into the marginal sinus around the foramen magnum joining the jugular foramen on each side. The transverse sinuses are correspondingly hypoplastic. |
Supratentorial Intradural Venous System
The venous drainage pattern of the supratentorial structures is described as having a superficial system and a deep system. This is a useful division, but there are some superficial areas of cortex that drain via veins of the deep system. In the setting of anomalous or pathologic venous flow, the distinction between the two systems becomes blurred. Nevertheless, where surgery is planned, it is important to be able to recognize the major veins and sinuses present and to describe their direction of flow. Sacrificing major cortical veins or subdural bridging veins carries some risk of venous infarction and is therefore kept to a minimum during surgery (Fig. 16-6).
Superficial Supratentorial Cortical Veins
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


