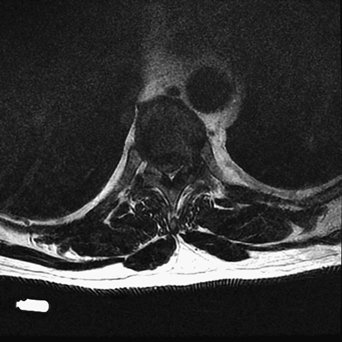
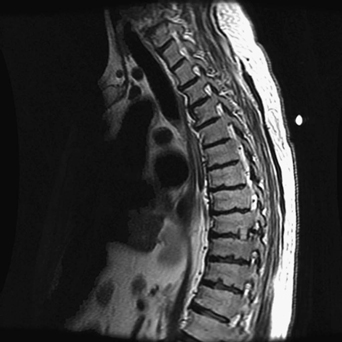
34 A 60-year-old man presented with progressive paraplegia and a thoracic sensory level. A thoracic magnetic resonance imaging (MRI) showed a T8-T9 disc with thecal sac compression (Figs. 34-1 and 34-2). FIGURE 34-1 Sagittal thoracic T2-weighted MRI showing a thoracic disc protrusion compressing the cord. Thoracic disc extrusion with cord compression A thoracic laminectomy and pediculectomy was performed to gain access to the disc space for its removal. FIGURE 34-2 Axial T2-weighted thoracic MRI demonstrating the circumferential cord compression. FIGURE 34-3 MRI of the thoracic spine is notable for rib graft insertion into the discectomized space after a mini-lateral extracavitary approach for thoracic discectomy. Thoracic discs are underdiagnosed, probably due to their rare nature and their presentation. The incidence is one in a million a year in the United States. Often the presentation emulates that of lumbar disc disease, with back and leg pain, and sometimes bowel and bladder difficulty. Additionally, thoracic discs can mimic abdominal pathology. The presence of myelopathy, a thoracic sensory level, and more proximal pain involvement can help differentiate thoracic from lumbar pathology on examination. T4 to T9 is a watershed area of blood supply to the spinal cord. This and the narrower kyphotic nature of the thoracic canal make cord compression in this region a serious problem. In addition, surgery on this area has a high potential morbidity for the aforementioned reasons and presents the challenge of lesion localization. There are several approaches one can take for a thoracic discectomy. Standard laminectomy is inappropriate and often mentioned in this setting only to be condemned; the high rate of morbidity stems from cord manipulation to get access to the disc space. One can use a dorsolateral approach-transpedicular or transfacetal to the disc. Although visualization is not complete here, these approaches are preferred by some due to their directness and familiarity to spine surgeons. The extra-cavitary approach is direct and lateral. This approach enables the surgeon to have good access to the pathology without the inherent risks of posterior approaches or the comorbidity attached to anterior ones; however, unfamil-iarity with this technique renders it unattractive to some. One can perform a mini-lateral extracavitary version using a small linear paramedian incision to access one or multiple thoracic discs. Rib graft can then be inserted into the disc space for fusion purposes. A postoperative MRI from such a case seen in Fig. 34-3. Anterior approaches include transthoracic, retro-pleural, and transsternal. Lateral and ventral approaches are now being done endoscopically to lessen the morbidity. A steep learning curve is expected. Levi N, Gjerris F, Dons K. Thoracic disc herniation. Unilateral transpedicular approach in 35 consecutive patients. J Neurosurg Sci 1999;43:37–43
Thoracic Disc
Presentation
Radiologic Findings

Diagnosis
Treatment
Discussion
SUGGESTED READING
< div class='tao-gold-member'>
Thoracic Disc
Only gold members can continue reading. Log In or Register to continue







Full access? Get Clinical Tree


