♦ Preoperative
Imaging
- Plain x-rays
- Determine location of pathology in relation to lower thoracic ribs
- Assess deformity and/or instability
- Determine location of pathology in relation to lower thoracic ribs
- Magnetic resonance imaging (MRI)
- Determine extent of neural element compression
- Computed tomography
- Evaluate bony anatomy
- Computed tomography/myelogram
- If MRI contraindicated
- Pulmonary function tests for patients with history of compromised pulmonary function
Operative Planning
- Patient counseling regarding risk, benefits, and postoperative course
Routine Equipment
- Basic spine tray including Kerrison rongeurs (2 to 4 mm)
- Thoracotomy tray including long curettes, rongeurs, and Cobb dissectors
- Table-mounted retractor (Thompson-Farley versus Omni-Tract)
- Cautery–monopolar with an extended tip and bipolar
- High-speed drill (e.g., Midas Rex)
- Headlight and loupe magnification
Special Equipment
- Cell Saver if significant blood loss anticipated in the absence of infection/neoplastic disease
- Microscope for intradural pathology
- Spinal instrumentation if reconstruction necessary
- Including ventral interbody strut and anterolateral tension band
- Bean bag for lateral positioning
- Compatible table for intraoperative imaging–x-ray versus fluoroscopy
Anesthetic Issues
- Appropriate venous and arterial line access
- Routine induction and intubation are performed.
- Foley catheter
- Perioperative antibiotics 30 minutes prior to skin incision
- Perioperative steroids for decompressive or intradural pathology
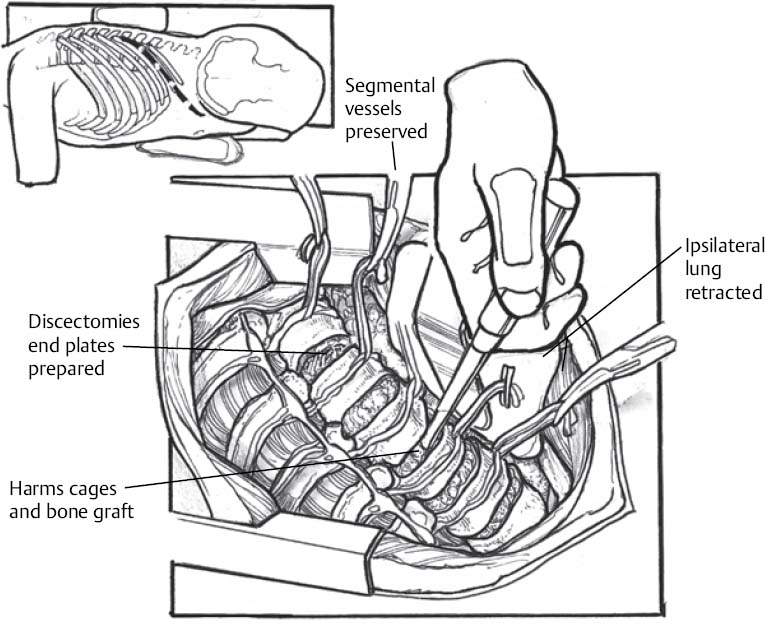
♦ Intraoperative (Fig. 112.1)
Positioning
- Lateral position with side determined by level and location of pathology
- Exposure of the ventral spine is generally easier from the left side because of the liver and inferior vena cava (IVC) on the right.
- Axillary role placed under dependent arm
- Free arm supported on pillow or armrest
- The lower leg is flexed at the hip and knee for stabilization and pillow placed between the legs
- Appropriate padding of all bony prominences and superficial peripheral nerves
Planning of Sterile Preparation
- Standard scrub and preparation
Planning of Incision
- For pathology from T10 to T12, the rib to be removed is typically two levels rostral to the pathology.
- The incision for exposure from T10–L2 extends from the posterior axillary line to the lateral border of the paraspinal muscle (~4 cm from midline) along the surface of the rib to be resected, approximately 10–14 cm.
- Intraoperative localization is performed by taping a radiopaque instrument along the rib to be resected, making sure that the rib overlies the level of pathology.
Exposure
- If unfamiliar with this exposure, one should consider incorporating the assistance of an approach surgeon.
- Superficial muscle layers are transected in line with the skin incision utilizing monopolar cautery.
- If resection of the lower ribs is required, a subperiosteal dissection of the intercostal muscles over approximately 10 cm of the exposed rib is performed.
- The rib is dissected free from the ventral endothoracic fascia with a Doyen dissector and resected, leaving the proximal 4 cm of the rib attached to the transverse process and vertebral body.
- The cut end of the rib is waxed. The resected bone is saved for grafting.
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continueRelated posts:

Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


