♦ Preoperative
Management Decisions
- Maintenance of neurologic and mechanical stability
- Prevent further instability, deformity, or segmental collapse while maintaining normal spinal mechanics
- Minimize the amount of fused levels to maintain maximum mobility
Advantage of an Anterior Approach
- Direct decompression the spinal canal
- Reconstruction of the anterior column and stabilization in one setting
♦ Intraoperative (Fig. 109.1)
Positioning
- Lung isolation with a double lumen endotracheal tube
- Lateral decubitus position, radiolucent table
- A left-sided approach is preferred for the treatment of pathologies from T4 to T8.
- A right-sided approach is preferred for exposing the thoracolumbar junction (T9 to L3).
- The upper arm is abducted and elevated so that it does not interfere with the placement and manipulation of the endoscope.
- The surgeon stands behind the patient.
Operative Planning
- The target area is projected onto the skin level under fluoroscopic control.
- The borders of the involved vertebra are marked on the skin.
- The working channel is centered over the target vertebra.
- The optical channel is placed between two and three intercostal spaces cranial to the target vertebra in the spinal axis.
- The approach for suction, irrigation, and retractor is placed ~5 to 10 cm anterior to the working and optical channels.
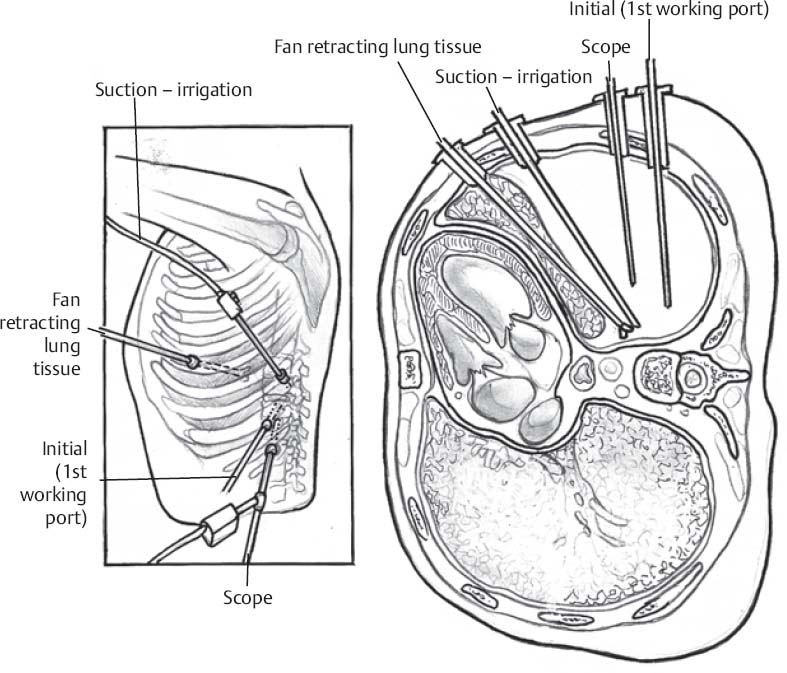
Placement of Portals
- The position of the portals in relation to one another and to the operating site on the spine influences the entire course of the operation.
- The operating portal is the first position to be marked exactly over the target area, and then, corresponding to this, the portal for the optic is drawn in over the spine, two or three intercostal spaces above the mark for the operating portal.
- Portal for suction and irrigation instruments is approximately four finger-breadths from the operating portal in a ventral and cranial direction.
- The portal for the diaphragm or lung retractor should be placed as far ventrally as possible to avoid instruments coming into conflict.
- Lung isolation should start prior to incision.
- Subsequently, the most cranial portal (optical channel) should be placed first.
- Through a 1.5-cm skin incision above the intercostal space, a muscle splitting technique is used to bluntly open into the intercostal space.
- A 10-mm trocar is inserted into the thoracic cavity; a 30-degree endoscope is inserted at a flat angle in the direction of the second trocar.
- Perforation of thoracic wall to insert the remaining trocars is performed under direct intrathoracic visualization through the scope.
Prevertebral Dissection and Diaphragm Detachment (if Needed for Exposure of the Thoracolumbar Junction)
- A fan retractor inserted through the anterior port can retract the diaphragm and expose the insertion of the diaphragm onto the spine.
- Total detachment of the diaphragm is not necessary for exposure of the thoracolumbar junction.
- A diaphragmatic opening of ~6 to 10 cm can expose the entire L2 vertebral body.
- The anterior circumference of the motion segment can be palpated with a blunt probe.
- The line of dissection for the diaphragm is marked with monopolar cauterization.
- The diaphragm is then incised using endoscissors.
- A rim of 1 cm is left on the spine to facilitate closure of the diaphragm at the end of the procedure.
- Retroperitoneal fat tissue is now exposed and mobilized from the anterior surface of the psoas insertions.
- The psoas muscle is dissected very carefully from the vertebral bodies in order not to damage the segmental blood vessels underneath.
- The retractor is placed into the diaphragmal gap.
Corpectomy and Decompression of the Spinal Canal
- The disc spaces are opened to define the borders. After, the fragmented parts of the vertebra(e) are removed.
- Resection close to the spinal canal is facilitated with the use of a highspeed burr.
- If decompression of the spinal canal is necessary, the lower border of the pedicle is identified and resected.
- The thecal sac can be identified. Further fragments can then be removed.
- Then, the necessary arthrodesis and fixation is accomplished.
♦ Postoperative
- The thoracic cavity is irrigated, and blood clots are removed.
- All patients who undergo this approach require insertion of a chest tube.
- The portals are closed after removal of the trocars.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue






