Chapter 61 Thoracoscopic Corpectomy and Reconstruction
Spinal instability caused by trauma or destructive disease has historically been treated through a dorsal approach. Purely dorsal techniques, however, often fail adequately to address ventrally located pathology. Dorsal decompression with thoracic laminectomy of ventral epidural masses has been associated with increased risk of injury to the spinal cord. Ventral spinal canal decompression through dorsal and even posterolateral approaches can be challenging and ineffective.1–3 Furthermore, dorsal instrumentation may not sufficiently stabilize a significantly disrupted ventral load-bearing spinal column.4,5
To more effectively and directly decompress and stabilize the ventral spine, ventral thoracotomy and thoracoabdominal techniques were developed.6,7 Although these approaches demonstrated improved outcomes and are an acceptable treatment modality for ventral thoracolumbar disease, the high access morbidity of these open procedures often results in post-thoracotomy pain syndromes, postoperative pneumothorax or pleural effusion, shoulder dysfunction, abdominal wall relaxation, and significant scarring of the chest wall.8
Spine surgeons have more recently adapted the minimally invasive thoracoscopic techniques that have been applied by thoracic surgeons for many years. Thoracoscopic spine surgery was first used for the treatment of thoracic disc herniations and traumatic fractures. With advances in thoracoscopic video technology, instrumentation, and instrument systems, thoracoscopic spine surgery has improved significantly, and its use has been expanded to include the treatment of most ventral thoracolumbar disorders, including trauma, tumor, and degenerative disease, as well as deformity correction in select cases.4,9–15
Specialized tools for endoscopic spine surgery are used to access the thoracic cavity through small chest incisions, and the surgery is performed under two-dimensional video guidance. Minimizing chest wall dissection and retraction through the use of small thoracoscopic incisions has significantly improved outcomes and reduced postoperative morbidity without compromising long-term successful fusion rates.9–11,16–18 The minimally invasive thoracoscopic approach can now be safely and effectively performed to treat disease that had previously required an open thoracotomy.
Advantages and Disadvantages
Several advantages are offered by the minimally invasive ventrolateral thoracoscopic approach over an open thoracotomy. Multiple vertebral levels and the ventral spinal canal can be visualized and treated without increasing surgical exposure when access ports are properly placed. The surgical field can be imaged with excellent resolution using modern high-definition endoscopic technology. The small intercostal incisions negate the need for rib resection and retraction, unlike open thoracotomy approaches, which necessitate large incisions, extensive dissection of intercostal muscles, rib resection, and retraction of the chest wall. The thoracoscopic approach is associated with reduced blood loss, need for blood transfusion,19 days of mechanical ventilation, perioperative wound pain, incidence of pulmonary and shoulder dysfunction, length of hospital stay, and days to rehabilitation.16–18
For most spine surgeons, the major disadvantage of the thoracoscopic approach is unfamiliarity with the technique and high technical demand. The operation is performed distant from the surgical site in two dimensions based solely on thoracoscopic image guidance, which requires most spine surgeons to acquire a new set of skills. Before operating on a patient, the surgeon must gain familiarity with the new technique in practical and didactic training sessions. The surgeon and operating room staff must overcome a steep learning curve while gaining familiarity with the approach, and this can initially increase operative times by several hours. Anesthesia monitoring and double-lumen ventilation may also increase operative times. Conversion to an open thoracotomy may be required with difficult cases or when intraoperative complications cannot be resolved with the thoracoscopic technique. Finally, extensive intrathoracic disease, whether pulmonary or spinal, may be difficult to address with the thoracoscopic approach.
Indications and Contraindications
The thoracoscopic approach is best suited for patients with thoracolumbar disease limited to one vertebral body and the ventral spinal canal between T3 and L3, although multiple levels may be treated. The most common indication for thoracoscopic spinal surgery is in the setting of trauma. Among patients with traumatic spinal injury, ventral spinal reconstruction for biomechanical instability is the most common surgical indication. Traumatic spinal instability may be secondary to fracture, injury to the intervertebral discs, or significant ligamentous disruption. The mainstay of treatment for thoracolumbar fractures is rigid fixation with transpedicular screw and rod constructs. The decision to add ventral column reconstruction is based on the load-bearing capacity of the injured spinal segment. The load-sharing classification system developed by McCormack et al.5 established a correlation between failure of dorsal short segment fixation and the characteristics of the most significantly injured vertebrae. Fractures with a high degree of vertebral body comminution, fragment apposition, and postoperative deformity correction were found to be at high risk for dorsal instrumentation failure. Thoracoscopic surgery for reconstruction of the ventral load-bearing elements is indicated in these patients. Although patients with neurologic deficits from fracture intrusion into the ventral spinal canal comprise a minor subgroup of patients with traumatic spine injury, they are also indicated for spinal canal decompression and ventral stabilization.
In cases of spinal tumor, thoracolumbar surgery is indicated for treatment of spinal instability, radiation treatment failures, most cases of spinal stenosis secondary to epidural tumor causing neural compression, and pain intractable to conservative measures or to obtain a histologic diagnosis.3,20–23 The thoracoscopic approach is indicated for resection of vertebral body tumors with or without ventral spinal canal involvement and for ventral column reconstruction with interbody placement and ventrolateral instrumentation.
Preoperative Assessment and Planning
Planning of Resection and Reconstruction
Detailed preoperative examination of the patient’s bony anatomy is important for planning the reconstruction. The appropriate lengths of the vertebral body screws are determined by measuring the widths of the vertebrae on the preoperative images. The height of the interbody is approximated by measuring the distance between the inferior end plate of the cranial level and the superior end plate of the caudal level. The plate dimensions can also be approximated preoperatively by measuring the distance between the lower third of the cranial vertebral body and the upper third of the caudal vertebral body. The extent of pathologic canal intrusion is also measured to determine the amount of bony resection needed for sufficient ventral spinal canal decompression.
Operative Technique
Thoracoscopic Instruments and Instrumentation Systems
In addition to specialized instruments, the MACS-TL ventrolateral thoracolumbar spinal implant (Aesculap, Tuttlingen, Germany) was specifically designed for thoracoscopic use (Fig. 61-1). It consists of a rigid plate that is secured to the ventrolateral vertebral body with two pairs of triangulated fixation screws for increased strength: two dorsal polyaxial screws and two ventral stabilizing screws. The screws are implanted into the normal vertebrae adjacent to the diseased vertebra(e). The fixation plate is then rigidly secured to the screws. The biomechanical properties of the MACS-TL plating system have been characterized in monosegmental and bisegmental partial and full corpectomy models both with and without dorsal ligamentous injury. Case series have also demonstrated its clinical efficacy.10,13,15,24–26

Localization
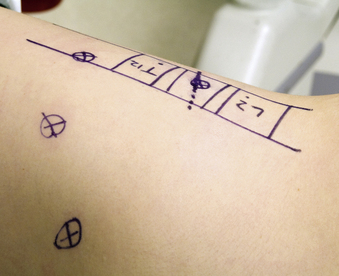
The relation of the spine and identified sites of the access portals is determined with intraoperative fluoroscopy. After optimal patient positioning, a lateral image centered over the pathologic area is obtained and projected orthograde onto the chest wall. The level of interest is often evident because of changes in spinal alignment and bony architecture. The skin is marked with a diagram outlining the vertebral bodies of the pathologic and adjacent levels by drawing the ventral and dorsal spinal lines and intervertebral discs. The four portal access sites are then marked (Fig. 61-2). The positioning of these portals determines working distances and is essential for proper retraction and intraoperative thoracoscopic image guidance.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


